Does Medicare Cover Nursing Home Care?
Does Medicare Cover Nursing Home Care?

Does Medicare Cover Nursing Home Care? The Direct Answer and Why the Details Change Everything
Medicare covers nursing home care only in narrow, specific circumstances — and the care most families mean when they say “nursing home” is almost entirely outside what Medicare pays for. Medicare Part A covers short-term skilled nursing facility care following a qualifying hospital stay, for up to 100 days per benefit period, only when the care required meets Medicare’s definition of “skilled.” It does not cover custodial care — the ongoing assistance with bathing, dressing, eating, toileting, mobility, and supervision that characterizes long-term nursing home residence for most elderly patients. For the first 20 days in a qualifying skilled nursing facility stay, Medicare covers the full cost with no copayment. For days 21 through 100, the patient owes a daily coinsurance of $217 in 2026. After day 100, Medicare pays nothing and the patient or family bears the full cost. This is the complete scope of Medicare’s nursing home coverage — and for most families navigating a serious care need, the gap between what Medicare covers and what long-term care actually costs is the most consequential financial planning gap in retirement. At Diversified Insurance Brokers, Jason Stolz, CLTC, CRPC, DIA, CAA helps clients understand exactly where Medicare ends and where long-term care planning must begin — identifying the appropriate coverage instruments before a care need arises rather than after. Whether Medicare covers long-term care broadly — beyond the skilled nursing facility question — is the foundational coverage question that every senior and every adult child planning for an aging parent needs to answer before assuming Medicare will handle it.
The Critical Distinction: Skilled Care vs. Custodial Care
Medicare’s coverage turns entirely on the classification of the care needed. Skilled care is care that must be performed by or under the supervision of licensed professionals — registered nurses administering IV medications, licensed therapists conducting physical or occupational rehabilitation, speech-language pathologists providing medically necessary therapy, or wound care requiring clinical expertise. When a patient needs skilled care and meets the qualifying conditions, Medicare Part A can pay for that care in a Medicare-certified skilled nursing facility for up to 100 days. Custodial care is fundamentally different: it is assistance with the activities of daily living — bathing, dressing, eating, toileting, transferring (moving from bed to chair), and continence management — that does not require professional clinical skill to perform safely. It also includes supervision for cognitive impairment or memory loss. Medicare does not cover custodial care regardless of where it is provided — whether in a nursing facility, an assisted living community, or the patient’s own home.
This distinction produces the most common and most painful surprise families encounter: a patient is discharged from the hospital to a skilled nursing facility for rehabilitation, Medicare pays as expected for the first weeks, and then the patient reaches a point where skilled rehabilitation is no longer medically necessary and the remaining need is custodial — help with daily activities and supervision. At that point, Medicare coverage ends, and the full cost of continued nursing home residence shifts to the patient or family. The transition from Medicare-covered to non-covered care can happen well before day 100 if the patient “plateaus” in therapy progress. A landmark federal court ruling — Jimmo v. Sebelius — clarified that Medicare must cover care needed to maintain a patient’s current condition or prevent decline, not only when active improvement is expected. In practice, however, coverage still ends when the qualifying conditions are no longer met, even if ongoing care is still needed. Long-term care insurance options at Diversified address the custodial care gap that Medicare leaves — the planning instrument specifically designed for the care that Medicare refuses to pay for. Long-term care insurance with shared spousal benefits specifically addresses the care cost planning for couples where either spouse may need extended custodial care during retirement.
Close the Long-Term Care Gap Before You Need It
We help seniors and families identify the right long-term care coverage strategy — before a care need forces decisions under time pressure.
Request Medicare & LTC GuidanceMedicare’s Skilled Nursing Facility Benefit — The Qualifying Rules and Cost Structure
| Coverage Period | What Medicare Pays (2026) | What the Patient Pays (2026) |
|---|---|---|
| Days 1–20 | 100% of covered costs — room (semi-private), meals, skilled nursing services, physical and occupational therapy, speech-language pathology, medications, medical supplies, and ambulance transport when other modes would endanger health | $0 copayment for the first 20 days if all qualifying conditions are met; the Part A benefit period deductible of $1,736 was applied at the preceding hospital admission, not at SNF admission |
| Days 21–100 | Medicare pays the covered costs above the daily coinsurance amount — if the facility charges more than Medicare’s allowed rate, the patient may also owe the difference depending on the facility’s participation agreement | $217 per day coinsurance in 2026; if the patient stays all 80 days (21 through 100), the total coinsurance owed exceeds $17,000; Medicare Supplement plans may cover part or all of this coinsurance depending on the Medigap plan type |
| Day 101 and beyond | $0 — Medicare pays nothing after day 100 in a benefit period; coverage cannot be extended regardless of continued skilled care need unless a new benefit period begins (requires 60+ consecutive days without inpatient or SNF care and a new qualifying hospital stay) | 100% of all costs — the full daily rate of the nursing facility, which for private-pay patients commonly ranges from $200 to $400+ per day in most markets; annual costs exceeding $80,000–$150,000 are common for long-term nursing home residence |
The cost table establishes the fundamental financial reality: even within the 100-day window where Medicare provides some coverage, the patient’s cost exposure from days 21 through 100 can exceed $17,000 in 2026 — and after day 100, the full cost of nursing home care falls entirely on the patient, family, Medicaid (if eligible after spending down assets), or a long-term care insurance policy. Medicare supplement plans for seniors — specifically Medigap policies — address the $217/day coinsurance exposure for days 21 through 100; Plan A, Plan B, and other Medigap structures have different provisions for SNF coinsurance coverage that should be confirmed when selecting a supplement plan. What long-term care insurance costs relative to the actual cost of care it covers establishes whether the premium investment makes financial sense for a specific planning situation — and for most families, the math strongly favors early planning when premiums are lower and health is more manageable.
The Three Qualifying Conditions — Where Most Families Get Surprised
Three qualifying conditions must all be met for Medicare to pay anything for skilled nursing facility care. Missing any one of them eliminates all Medicare coverage for that stay, regardless of the severity of the care need or the patient’s Medicare enrollment status.
Condition One: The 3-Day Inpatient Hospital Stay
Medicare requires a qualifying inpatient hospital stay of at least three consecutive days before SNF coverage can begin. The three days are counted as inpatient days — the day of discharge does not count, and time spent in the hospital under observation status does not count toward the three-day requirement. This observation status trap is the most common reason families lose expected SNF coverage: a patient spends four days in the hospital but two of those days were classified as observation rather than inpatient admission, leaving only two qualifying inpatient days — one short of the three required. The patient and family may be unaware of the observation classification until discharge, at which point the SNF admission proceeds but Medicare coverage is not triggered. A 2026 CMS demonstration program began waiving the 3-day rule for certain surgical procedures through 2030 — but the general rule remains in effect for all other admissions and represents a genuine planning consideration for anyone managing a hospital stay that might be followed by SNF rehabilitation. Hospital indemnity insurance for observation stays specifically addresses the cost-sharing exposure that arises when hospital time is classified as observation rather than inpatient — the supplemental coverage that applies precisely in the scenario where the Medicare SNF benefit is not triggered. Hospital indemnity for ER and urgent care visits is the complementary coverage for the acute care phase that precedes a potential SNF admission.
Condition Two: Entry Into SNF Within 30 Days of Hospital Discharge
Medicare requires that the skilled nursing facility admission occur within 30 days of the qualifying hospital discharge. If the patient returns home after discharge and then develops a care need requiring SNF admission more than 30 days after the hospital stay, the SNF stay does not qualify under the original hospital stay’s benefit. A new qualifying hospital admission would be required. This 30-day window creates a planning consideration for patients who are discharged to home rather than directly to SNF rehabilitation — if their recovery requires SNF care within the 30-day window, Medicare covers it; if the need arises after the window, it does not. Hospital indemnity for Medicare Advantage members addresses the broader cost-sharing structure that MA plans apply to SNF stays — which may differ from Original Medicare’s structure in ways that affect out-of-pocket exposure.
Condition Three: Medicare-Certified Facility and Medically Necessary Skilled Care
The SNF must be Medicare-certified — not all nursing facilities participate in Medicare, and a non-participating facility produces no Medicare coverage regardless of how the patient arrived. The care required must be medically necessary skilled care, not custodial assistance. Medicare’s determination of medical necessity can end before the 100-day limit if the treating team determines that skilled care is no longer required — even if the patient still has significant care needs that are custodial rather than skilled in character. Confirming Medicare certification before selecting a SNF for post-hospital rehabilitation, and understanding what happens when skilled care need ends while custodial care need continues, are the two practical planning questions that the 3-day qualification system creates for most families. Annuities with long-term care benefits provide an insurance-based funding mechanism for the custodial care costs that begin when Medicare coverage ends — a single contract that serves both the retirement income objective and the care cost protection objective. Non-qualified long-term care annuities specifically address this dual-purpose structure for non-qualified retirement assets.
What Medicare Does Not Cover — and What Does
Medicare does not cover long-term custodial nursing home care under any circumstances. It does not cover room and board in an assisted living facility, memory care unit, or residential care community — even if skilled care is also provided in that setting. It does not cover personal care assistants, adult day care, or in-home custodial assistance beyond the narrow skilled home health benefit. The funding sources for long-term custodial care when Medicare does not apply are: personal savings and assets (spend-down), Medicaid (which requires meeting strict income and asset eligibility thresholds after spending down), long-term care insurance (standalone or hybrid), annuities with long-term care riders, life insurance with chronic illness or long-term care riders, and reverse mortgage proceeds for homeowners. Each of these has different eligibility requirements, tax treatment, and planning implications. Hybrid life insurance with long-term care benefits combines permanent life insurance with a long-term care benefit in a single contract — addressing two distinct risks with one premium payment. Life insurance with chronic illness riders provides living benefit access from an existing life policy when a qualifying chronic illness requires long-term care — a feature built into many current permanent life contracts. Long-term care insurance options after age 80 address the narrower market available for buyers who have delayed the long-term care coverage decision into the oldest age brackets — where options are more limited but coverage is still available through select carriers.
The Retirement Income Foundation That Makes Care Planning Sustainable
Long-term care planning does not exist in isolation — it requires a sustainable retirement income foundation that can support care costs without depleting the household’s complete asset base. Social Security planning guidanceSocial Security planning guidance and maximizing Social Security benefits establish the income floor that determines how much retirement income remains available for care cost funding or insurance premium payments after essential household expenses are covered. How Social Security and annuities work together in a retirement income plan is the complete income architecture within which long-term care planning costs must be sustainably budgeted. Annuities for conservative investors represent the guaranteed income vehicle that makes fixed monthly insurance premiums — including long-term care insurance premiums — reliably affordable regardless of market conditions. Guaranteed income from annuities and annuity income as a monthly retirement cash flow source provide the income planning tools that determine whether care cost planning fits within the household budget without requiring asset liquidation. The best annuity for guaranteed retirement income from a specific accumulated base is the specific product comparison that Diversified conducts across 100+ carriers when designing the income foundation for a care-cost-aware retirement plan. The annuity rescue plan reviews existing annuity and insurance positions together — confirming that the complete protection architecture, including long-term care coverage, is optimized for current needs. What annuity guarantees mean at the contractual level provides the product security context for buyers evaluating annuity-based long-term care funding. Current fixed annuity rates and the fundamentals of how annuities work provide the background knowledge for buyers approaching the annuity-based long-term care funding question for the first time. Disability insurance for working buyers addresses the income replacement dimension of a health event that precedes retirement — protecting the income that funds all future care cost planning. Whether life insurance is still needed in retirement addresses the life insurance dimension of the complete senior protection portfolio alongside the long-term care planning need. Life insurance options over 50 and burial insurance for seniors frame the life insurance and final expense protection that exist alongside the long-term care coverage in a complete senior financial plan. Final expense whole life insurance specifically addresses the funeral cost protection that complements long-term care coverage at the end-of-life planning stage. Whether working past 65 affects Social Security benefits and the Medicare enrollment timing it creates is the pre-retirement planning context that directly precedes the Medicare and long-term care planning decisions addressed on this page. Annuity strategies for early retirees addresses care cost planning for buyers who retire before traditional retirement age, where the longer potential distribution period and earlier Medicare access questions make long-term care planning particularly consequential.
Understand What Medicare Covers — and Plan for What It Doesn’t
We help seniors and families map the Medicare benefit, identify the long-term care coverage gap, and design a sustainable plan before a care need forces the decisions.
Request Medicare Guidance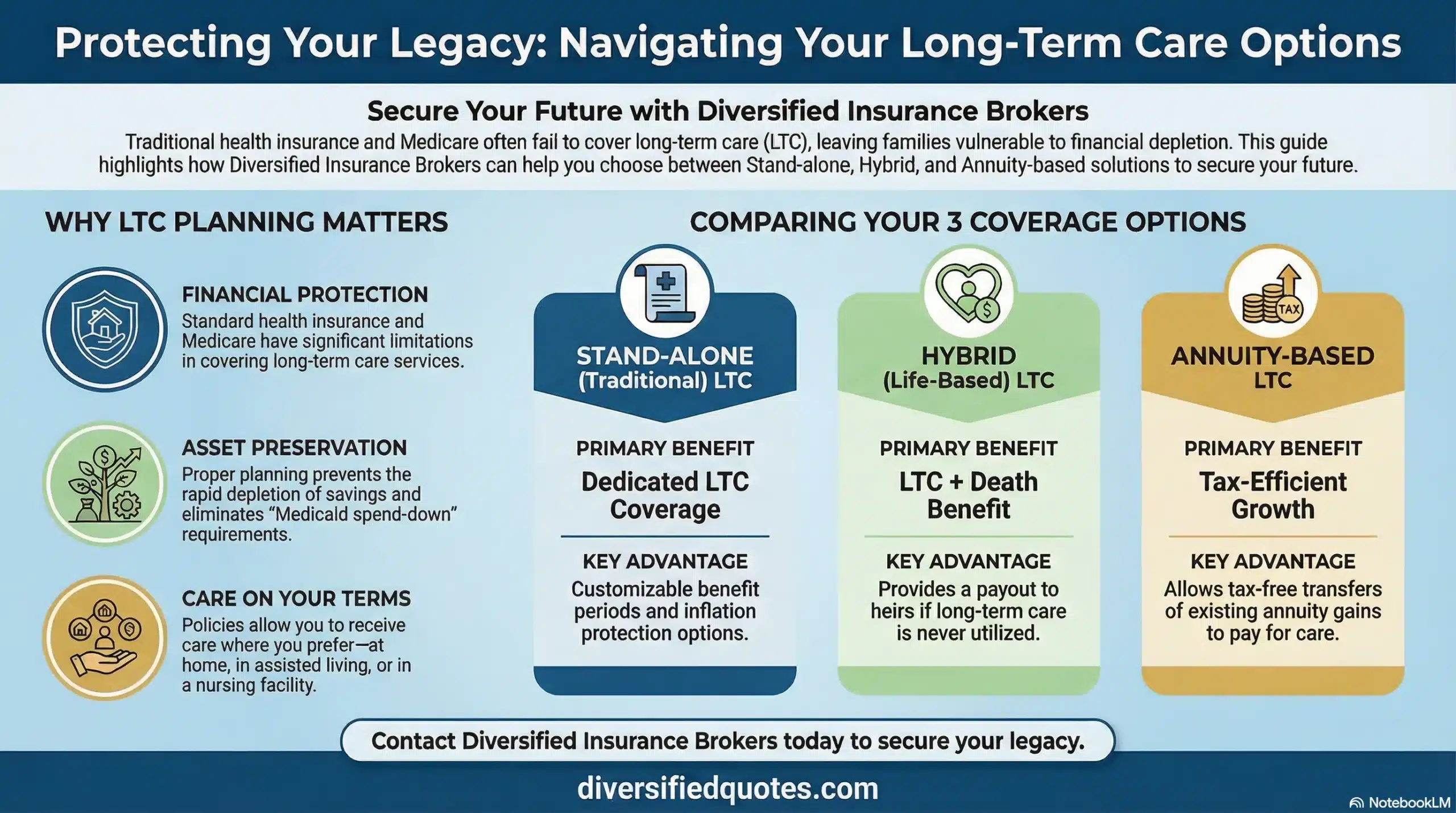
Questions now? Call 800-533-5969
FAQs: Does Medicare Cover Nursing Home Care?
My parent was in the hospital for four days but left without Medicare covering the SNF — why?
The most likely explanation is that some or all of the hospital time was classified as observation status rather than inpatient admission. Observation is an outpatient classification — even if the patient occupies a hospital bed, receives tests, and stays overnight, days under observation status do not count toward the three qualifying inpatient days required for Medicare SNF coverage. If your parent spent two days under observation and two days as an inpatient, only the two inpatient days count — one short of the required three. Families frequently are not informed of the observation classification until discharge, at which point SNF admission proceeds but Medicare coverage does not follow.
Medicare beneficiaries now have the right to appeal a denial of SNF coverage resulting from observation status reclassification. If the hospital failed to properly notify the patient of their outpatient observation status during the stay — as required under the Medicare Outpatient Observation Notice rule — there may also be grounds to contest the classification. Reviewing the hospital billing records to confirm the admission and observation day breakdown is the first step in understanding why SNF coverage was not triggered.
Can Medicare stop covering a SNF stay before 100 days?
Yes — Medicare can and regularly does stop covering SNF stays well before the 100-day limit. Coverage ends when the patient no longer requires medically necessary skilled care, regardless of how many days of the 100-day benefit remain. If the therapy team determines that the patient has reached the point where further skilled therapy or nursing is not medically necessary, Medicare will issue a notice that coverage is ending — typically with at least two days’ advance notice. The patient can request a review through the Beneficiary and Family Centered Care Quality Improvement Organization (BFCC-QIO), which can provide an independent determination of whether coverage should continue.
The landmark Jimmo v. Sebelius settlement confirmed that Medicare must cover care needed to maintain a patient’s current condition or slow decline — not only when active improvement is expected. If the SNF has been applying an “improvement standard” to end coverage — denying coverage because the patient is not making measurable progress in therapy — that is incorrect and the patient has grounds to appeal. In practice, appeals often succeed when the care need involves maintenance rather than improvement, particularly for patients with chronic or degenerative conditions where the goal of skilled therapy is preventing decline rather than achieving measurable gains.
Does Medicare Advantage cover nursing home stays differently than Original Medicare?
Medicare Advantage plans are required to cover at least the same benefits as Original Medicare Part A and Part B — which means every MA plan must cover SNF care on at least the same terms as Original Medicare. In practice, MA plans may structure the cost-sharing differently: some plans have lower daily copays for SNF days 21–100 than Original Medicare’s $217/day (2026), while others may have higher copays or require prior authorization before the SNF admission is approved as a covered stay. Prior authorization is the most significant operational difference — some MA plans require a review and approval before the SNF admission is confirmed as covered, which can create coordination challenges when a hospital discharge to SNF is time-sensitive.
Some MA plans also define the network of SNFs where coverage applies — out-of-network SNF admissions may be covered at reduced levels or may require prior approval under emergency provisions. Confirming that the specific SNF the patient or family prefers is in-network before discharge is an important planning step for MA beneficiaries that does not apply to Original Medicare beneficiaries, who can use any Medicare-certified SNF. The SNF benefit under MA also counts toward the plan’s maximum out-of-pocket limit, which Original Medicare Part A does not have — providing a ceiling on SNF cost-sharing for MA members that Original Medicare does not provide without a Medigap supplement plan.
What happens after Medicare stops paying for the nursing home — what are the options?
When Medicare coverage ends — either at the 100-day limit or earlier when skilled care is no longer required — the patient and family face the full cost of continued nursing home residence, which commonly ranges from $200 to $400 or more per day in most U.S. markets. The funding options at that point are: personal savings and liquid assets held by the patient; long-term care insurance if a policy was purchased before the need arose; an annuity with a long-term care benefit rider if one is in force; proceeds from a life insurance policy with a chronic illness or long-term care rider; Medicaid, if the patient qualifies after spending down countable assets to the applicable eligibility threshold; and in some cases, family support or reverse mortgage proceeds for homeowners who have not yet tapped home equity.
Medicaid is the public program that pays for long-term custodial nursing home care for patients who meet income and asset eligibility requirements — but Medicaid eligibility requires spending down most countable assets before coverage begins, which can eliminate the financial legacy the patient and family spent decades accumulating. Long-term care insurance and annuity-based long-term care benefits address the same care cost need as Medicaid but without the asset spend-down requirement — protecting the household’s assets while funding care. The planning decision between these options is best made years before a care need arises, when health permits underwriting approval and premium levels reflect the applicant’s younger age and healthier status.
Does a Medigap (Medicare Supplement) plan cover the SNF coinsurance?
Most Medicare Supplement (Medigap) plans cover part or all of the skilled nursing facility daily coinsurance for days 21 through 100. The amount of coverage depends on the specific Medigap plan type: Plan C and Plan F (available to those who became eligible for Medicare before January 1, 2020) cover 100% of the SNF coinsurance. Plans G, D, and several others also cover 100% of the SNF coinsurance. Plan A and Plan B do not include SNF coinsurance coverage. Plan K covers 50% and Plan L covers 75% of the SNF coinsurance. Confirming whether the specific Medigap plan held covers the SNF coinsurance — and at what percentage — is an important benefit review for any Medicare beneficiary who is or may be facing a SNF stay.
For beneficiaries who do not have a Medigap plan, the $217/day coinsurance for days 21–100 accumulates rapidly — staying the full 80 days from day 21 through day 100 produces a coinsurance obligation exceeding $17,000 in 2026. Medigap plans that cover this coinsurance protect against that specific exposure, though they do not address the post-100-day custodial care cost that is the larger and longer-lasting financial risk. The Medigap SNF coinsurance benefit is only relevant during the limited window when Medicare’s skilled care benefit applies — it has no function once the patient transitions to custodial care that Medicare does not cover.
How does a benefit period work for Medicare SNF coverage?
A Medicare benefit period begins the day a patient is admitted as a hospital inpatient and ends when the patient has been out of the hospital and has not received skilled care in a SNF for 60 consecutive days. Within a single benefit period, Medicare’s SNF benefit covers up to 100 days — days 1–20 at no cost and days 21–100 with the daily coinsurance. Once the patient is discharged and remains out of inpatient hospital or SNF care for 60 consecutive days, the benefit period ends and a new one can begin with the next qualifying hospital admission. There is no limit to the number of benefit periods a Medicare beneficiary can have over their lifetime — but each new benefit period requires a new qualifying hospital admission and resets the 100-day SNF benefit from the beginning.
The new benefit period also resets the Part A deductible — the patient owes a new $1,736 deductible (2026) at the start of each new inpatient hospital benefit period. Patients who cycle in and out of hospital and SNF care over a period of years may accumulate multiple deductibles if each new episode begins a new benefit period. The 60-day gap requirement means a patient who is discharged from SNF care and readmitted to the hospital within 60 days is still in the original benefit period, with the remaining unused days of the original 100-day benefit potentially still available for a subsequent SNF stay — though a new 3-day hospital stay would still be required for the SNF benefit to apply to the second stay within the same benefit period.
About the Author:
Tonia Pettitt, CMIP©, (NPN 14374308), is a seasoned Medicare specialist with more than 40 years of hands-on experience guiding individuals and families through the complexities of Medicare planning. As a senior advisor with the nationally licensed independent agency Diversified Insurance Brokers, Tonia provides clear, dependable guidance across all areas of Medicare—including Medicare Advantage, Medicare Supplement (Medigap), and Part D prescription coverage. Leveraging active contracts with dozens of highly rated insurance carriers, she helps clients compare options objectively and secure the most suitable coverage for their health and budget.
Known for her patient, education-first approach, Tonia has built a reputation as a trusted resource for retirees seeking reliable, unbiased Medicare support. With four decades of experience across evolving Medicare laws, carrier changes, and plan structures, she brings unmatched insight to every client conversation—ensuring clients feel confident, protected, and fully prepared for each stage of their retirement healthcare journey.
Explore More Medicare Options: Browse our complete guide to How Does Medicare Work? — covering Medicare Parts A, B, C & D explained — coverage, costs & how it all fits together.
Last Reviewed: June 9, 2026 |
Reviewed by: Tonia Pettitt, CMIP©
Medicare Specialist, Diversified Insurance Brokers, Inc. | NPN: 14374308 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Fact Checked by: Jason Stolz, CLTC, CRPC, DIA, CAA
Chief Underwriter, Diversified Insurance Brokers, Inc. | NPN: 20471358 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Editorial Standards: Diversified Insurance Brokers maintains rigorous editorial standards to ensure accuracy, clarity, and independence in all content. Learn more about our editorial standards and commitment to transparency.
