Does Medicare Cover Long Term Care
Does Medicare Cover Long Term Care

Does Medicare cover long term care? The answer that most retirees and their families discover — often at exactly the wrong moment, during a hospital discharge or a sudden health transition — is no. Medicare does not cover long-term custodial care. Not in a nursing home. Not in an assisted living facility. Not at home when what is needed is ongoing help with bathing, dressing, eating, or moving safely. Medicare is a health insurance program built around acute medical needs and short-term recovery. It was not designed to fund the months or years of daily personal assistance that characterize what most people think of when they picture needing long-term care in retirement. The gap between what Medicare covers and what long-term care actually costs is one of the most significant unaddressed financial risks in American retirement planning — and understanding exactly where Medicare stops is the essential first step toward building a plan that protects against what it leaves exposed.
At Diversified Insurance Brokers, Medicare specialist Tonia Pettitt, CMIP — with more than 40 years of experience guiding retirees through Medicare’s rules and coverage boundaries — helps families understand precisely what Medicare does and does not provide for long-term care situations. This page covers Medicare’s actual coverage mechanics, the specific conditions that do and do not trigger what limited skilled nursing coverage Medicare provides, why Medigap supplements and Medicare Advantage plans do not solve the long-term custodial care gap, what Medicaid requires before it steps in, and how long-term care insurance fills the gap that Medicare definitively cannot. Our resource on how does Medicare work covers the foundational Medicare framework, and our resource on are Medicare and long-term care insurance the same addresses the confusion between the two programs directly.
Understand the Gap Between Medicare and Long-Term Care
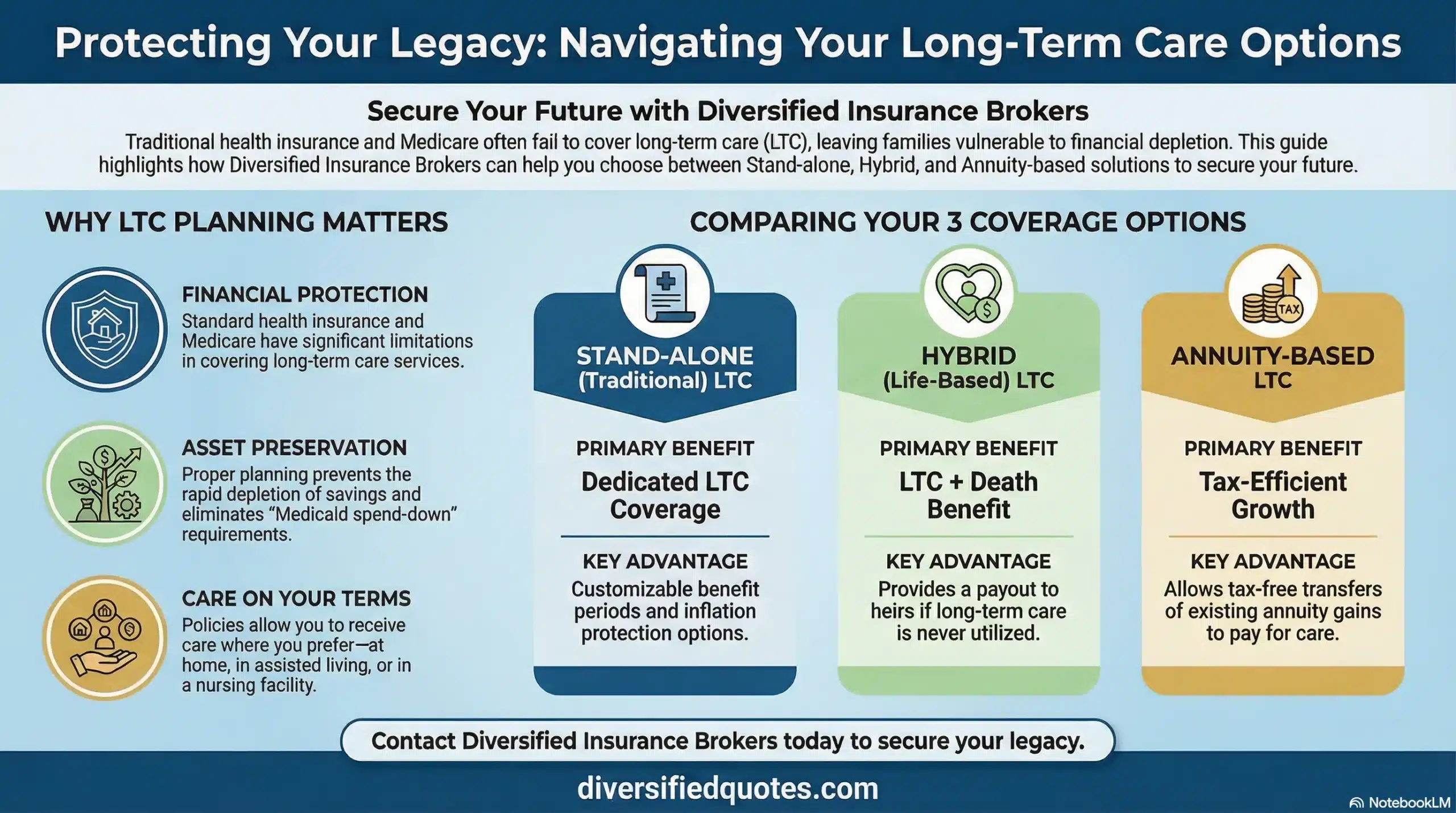
We compare long-term care coverage options — traditional LTC, hybrid life/LTC, and annuity-based LTC designs — and show exactly how each fills the gap Medicare leaves, for your age, health, and planning goals.
Request My LTC Coverage ReviewThe Direct Answer: What Medicare Covers for Long-Term Care — and What It Doesn’t
Does Medicare cover long term care in a nursing home or assisted living facility? No — not for custodial care purposes. Does Medicare cover home aides who help with bathing, dressing, or meal preparation on an ongoing basis? No. Does Medicare cover memory care for Alzheimer’s or dementia on an extended basis? No. Medicare’s role in long-term care is narrow, specific, and time-limited — and the conditions that must be met to trigger even that narrow coverage are frequently misunderstood by the retirees and families who discover they needed that understanding before a care crisis arrived rather than during one.
What Medicare does cover in the long-term care adjacent space is short-term skilled nursing care following a qualifying hospital admission, and limited home health services tied to a skilled care need ordered by a physician. These are medically defined, time-limited benefits connected to recovery from an acute medical event — not long-term support for ongoing functional limitations or cognitive decline. The moment a person’s care needs transition from “recovering from a medical event” to “needing ongoing help with daily activities,” Medicare’s coverage framework is essentially over. The ongoing help — which is the heart of what most people mean when they say “long-term care” — falls entirely outside what Medicare pays for.
Medicare’s Skilled Nursing Facility Coverage — The 100-Day Rule in Full Detail
| SNF Stay Period | Medicare Pays | You Pay (2025) | Key Condition |
|---|---|---|---|
| Days 1 through 20 | 100% of covered services | $0 | Qualifying 3-day inpatient hospital stay; admission to Medicare-certified SNF; daily skilled care medically necessary |
| Days 21 through 100 | Remaining covered costs above the daily copayment | $209.50 per day (2025) | Continued daily skilled care medically necessary; same condition related to hospitalizing diagnosis |
| After Day 100 | Nothing — zero coverage for any SNF costs | 100% of all SNF costs — private room ~$10,646/month; semi-private ~$9,277/month (2025 medians) | No Medicare coverage regardless of medical condition |
| Custodial care only (any point) | Nothing — not covered at any point | 100% of all costs | Custodial care — help with ADLs without skilled nursing component — is not covered by Medicare at any time |
| Assisted living / Memory care | Nothing — not a Medicare-covered setting | 100% of all costs — typically $4,000–$8,000+/month depending on location and level of care | Assisted living and memory care are not covered by Medicare under any conditions |
The table reveals the reality of does Medicare cover long term care in precise terms: the maximum coverage Medicare provides in a skilled nursing facility is 100 days per benefit period — and that coverage terminates at Day 100 completely, with no extended coverage available regardless of ongoing care needs. The copayment in Days 21 through 100 of $209.50 per day in 2025 means the household’s out-of-pocket exposure during that phase alone is potentially $16,969 over the 80-day period — a significant cost that accumulates even before the Day 100 cutoff when full private-pay costs begin. After Day 100, the median monthly cost for a private nursing home room is approximately $10,646, and for a semi-private room approximately $9,277 as of 2025 data. These costs continue as long as the person needs care — weeks, months, or years — with no Medicare contribution. Our resource on Medicare Part A explained covers the hospital and skilled nursing benefit structure in detail, and our resource on cost of long-term care by state calculator provides the state-specific cost data that shows what this gap actually costs in specific markets.
The Qualifying Hospital Stay Requirement — What Counts and What Doesn’t
Does Medicare cover long term care in a skilled nursing facility only after a qualifying hospital stay? Yes — and the requirements for that qualifying hospital stay are more stringent than most retirees realize, creating a common trap that denies SNF coverage to patients who assumed they qualified.
The qualifying hospital stay requires a minimum of three consecutive days as a formal inpatient in a Medicare-participating hospital — and the day of discharge does not count toward the three-day minimum. This means a patient must be formally admitted and remain for at least four calendar days (three full inpatient days plus the discharge day) to create the qualifying stay. The patient must then be admitted to a Medicare-certified skilled nursing facility within 30 days of hospital discharge for a condition that was treated during the hospital stay, and the SNF care must require skilled services — not merely custodial assistance.
The “observation status” classification creates one of the most consequential and frequently misunderstood gaps in Medicare’s coverage framework. Patients who are placed in a hospital bed under “observation status” rather than formal inpatient admission are classified as outpatients for Medicare purposes, even though they are physically in a hospital room and may stay for multiple nights. Observation status days do not count toward the 3-day inpatient qualifying requirement, even if the patient occupies a hospital bed for several nights under observation. A patient who spends 4 days in a hospital but only 2 of those days as a formally admitted inpatient does not have the qualifying hospital stay — and when they are discharged to a skilled nursing facility, Medicare’s SNF coverage does not apply. The resulting bill for the entire SNF stay falls to the patient as private pay, creating a financial surprise that families frequently describe as one of the most jarring and unexpected experiences in their Medicare journey. Our resource on Medicare enrollment mistakes to avoid covers the observation status trap among other common and costly Medicare misconceptions.
Skilled vs Custodial Care — The Critical Distinction Medicare Draws
The reason does Medicare cover long term care has such a categorical answer is rooted in a single definitional distinction that Medicare draws between two types of care: skilled care and custodial care. Every aspect of Medicare’s limited long-term care adjacent coverage depends on this distinction, and the moment a person’s care needs move from the skilled category to the custodial category, Medicare’s coverage obligation ends regardless of how much the person needs ongoing help.
Skilled care, in Medicare’s framework, means care that requires the skills of licensed medical professionals — registered nurses, physical therapists, occupational therapists, speech therapists, or other similarly licensed practitioners — and that is medically necessary and ordered by a physician. Skilled nursing care in a Medicare context includes wound care, IV therapy, complex medication management, post-surgical monitoring, catheter care, or intensive rehabilitation following a stroke or orthopedic procedure. The defining characteristics are medical complexity, licensed professional involvement, and an expectation of measurable improvement or maintenance of a medical condition.
Custodial care means ongoing assistance with the Activities of Daily Living — bathing, dressing, eating, toileting, transferring from bed to chair, managing continence — and with instrumental activities like meal preparation, medication management, and safe navigation of the home environment. Custodial care can be provided in a nursing home, an assisted living facility, a memory care community, or at home by a professional caregiver. The defining characteristics of custodial care are ongoing rather than time-limited need, personal rather than medical in nature, and not requiring the skills of licensed medical professionals on a daily basis. Our resource on what are Activities of Daily Living covers the specific ADL definitions that determine benefit eligibility under long-term care insurance policies — the same framework used to determine when LTC insurance begins paying for the care that Medicare does not cover.
The critical planning implication of this distinction is that a person can be genuinely unable to care for themselves — physically dependent on others for basic daily functions — without qualifying for a single day of Medicare-funded skilled nursing or home health care. The inability to dress, bathe, or prepare meals independently is not a Medicare-covered care need. It is a long-term care need, and it must be funded from personal savings, Medicaid (after asset spend-down), or long-term care insurance. This is the core of why does Medicare cover long term care is such an important question for retirement planning — because the vast majority of what people actually need when they need ongoing care in old age is custodial in nature, not skilled, and therefore entirely outside Medicare’s coverage framework.
What Medicare Home Health Coverage Actually Includes — and Its Limits
Medicare does provide some home health coverage, and this is the area where confusion most frequently arises about whether does Medicare cover long term care in a home setting. Medicare Part B covers home health services — but only under specific conditions that distinguish it sharply from the ongoing custodial home care that most people associate with aging at home.
Medicare-covered home health services require a physician’s order, must be medically necessary, and must include a skilled component — skilled nursing visits, physical therapy, occupational therapy, or speech therapy ordered for a specific medical condition. Medicare home health is designed for intermittent, part-time skilled care in the home — not for ongoing daily personal care or full-time home health aide services. The home health aide services that Medicare covers in this context are limited to situations where skilled care is also being received and the aide services are incidental to the skilled care. When the skilled care component ends — when the therapist determines that measurable goals have been achieved or that progress has plateaued — the entire home health benefit ends, including any aide services that were accompanying the skilled care.
Critically, Medicare home health coverage requires that the beneficiary be homebound — defined as leaving home requiring considerable effort, a condition that limits eligibility to those who are genuinely confined to the home by illness or injury. And even for those who meet the homebound requirement and have a qualifying skilled care need, the aide hours covered are not designed to substitute for 24-hour home care or full-time personal care assistance. The person who needs a home health aide for 8 hours per day to safely manage at home while cognitively or physically declining will not find that level of assistance within Medicare’s home health benefit. Our resource on Medicare Part B explained covers the outpatient benefit framework including home health coverage.
Does Medicare Advantage Cover Long-Term Care?
Does Medicare cover long term care through Medicare Advantage plans? The answer remains no for custodial care — with very limited exceptions that do not constitute a true long-term care solution. Medicare Advantage plans (Medicare Part C) are required to cover everything that Original Medicare Parts A and B cover, which means they cover the same narrow skilled nursing benefit and the same limited home health benefit with the same medical necessity requirements. They do not cover custodial care, assisted living, memory care, or ongoing home aide services simply because those are not Medicare-covered services in any plan structure.
Some Medicare Advantage plans — particularly Chronic Special Needs Plans (C-SNPs) and plans that include Special Supplemental Benefits for the Chronically Ill (SSBCI) — may provide modest additional in-home supports, transportation assistance, meal delivery, or caregiver respite that can be genuinely helpful. These supplemental benefits can reduce some of the daily friction and cost burden for members managing chronic conditions at home, and they are a meaningful part of Medicare Advantage’s value proposition for specific health situations. But they are supplemental benefits with defined limits and eligibility requirements — not a true long-term custodial care funding solution. A benefit that provides 12 in-home support visits per year does not address the need for 20+ hours per week of home care for a person with advancing dementia. Our resource on Medicare for people with chronic conditions covers the Medicare Advantage C-SNP programs and what they genuinely provide, and our resource on Medicare Advantage versus Medicare supplement comparison covers the structural differences between the two coverage approaches for the broader Medicare decision.
Does Medigap (Medicare Supplement) Cover Long-Term Care?
Does Medicare cover long term care through Medigap supplements? No. Medicare Supplement insurance (Medigap) covers cost-sharing gaps in Original Medicare — the deductibles, copayments, and coinsurance that Medicare does not pay. What Medigap does not do is extend Medicare’s coverage to services that Medicare does not cover at all. Since Medicare does not cover custodial long-term care, Medigap does not cover it either — by definition, because Medigap can only supplement benefits that exist within Original Medicare’s framework.
There is one specific area where Medigap does provide meaningful value related to skilled nursing: many Medigap plans, including Plan G — the most comprehensive plan currently available to new Medicare beneficiaries — cover the skilled nursing facility coinsurance for Days 21 through 100. In 2025, that coinsurance is $209.50 per day. A Medigap Plan G policyholder in a Medicare-qualified SNF stay for Days 21 through 100 would have the $209.50 per day copayment covered by the supplement, potentially reducing out-of-pocket costs by up to $16,760 over that 80-day period. This is a genuine and meaningful cost protection for the short-term skilled nursing scenario — but it remains irrelevant to the question of does Medicare cover long term care for custodial purposes, because neither Medicare nor Medigap covers custodial care at any cost-sharing level. Our resource on best Medicare supplement plans for seniors covers Medigap plan comparison, and our resource on Medicare supplement coverage for cancer treatment illustrates how Medigap functions for high-cost medical scenarios even though it cannot address the custodial care gap.
Medicaid and Long-Term Care — The Safety Net That Requires Spending Down
Medicaid does cover long-term custodial care — but only after the applicant has spent down assets to meet Medicaid’s strict income and asset eligibility requirements. Medicaid is a needs-based program, and qualifying for Medicaid long-term care coverage typically requires spending most of one’s savings, liquidating assets, and meeting state-specific asset limits that vary but are generally very low for single individuals. A married couple has some protections — called Community Spouse Resource Allowance (CSRA) provisions — that allow the healthy spouse to retain a defined portion of assets while the care-receiving spouse receives Medicaid, but these protections have limits and the specifics vary by state.
Beyond the asset spend-down requirement, Medicaid long-term care limits facility choice to those that accept Medicaid payment — which may exclude preferred facilities, higher-quality nursing homes, and specific assisted living communities in some markets. Waiting lists for Medicaid home and community-based waiver services can be substantial in some states. And the unpredictability of state Medicaid program rules, which can change through legislative action, creates planning uncertainty for households that plan to rely on Medicaid as their primary long-term care funding mechanism. The household that plans proactively for long-term care with private insurance is not planning to avoid Medicaid at any cost — it is planning to maintain choice, control, and quality of care during a care event rather than making those choices by default based on whatever Medicaid-funded options are available when need arrives. Our resource on self-insured long-term care covers the analysis of when self-funding is realistic and when Medicaid spend-down becomes the unintended consequence of planning to self-insure.
How Long-Term Care Insurance Fills the Gap Medicare Leaves
Long-term care insurance is specifically designed to cover what does Medicare cover long term care analysis reveals Medicare does not: ongoing custodial care at home, in assisted living, in memory care, in adult day programs, and in skilled nursing facilities after Medicare’s benefit period ends. Where Medicare requires medical necessity and skilled care, long-term care insurance is triggered by the functional or cognitive need that characterizes genuine long-term dependence — the inability to perform 2 or more Activities of Daily Living, or the presence of severe cognitive impairment requiring substantial supervision. These triggers align with what families actually experience when a care need arrives, not with what a physician must certify as medically necessary skilled treatment.
The coverage long-term care insurance provides is designed for the scenario that Medicare cannot address: the person who no longer needs daily IV therapy but still needs help getting out of bed each morning, the person who has plateaued in physical therapy but cannot safely prepare meals or manage medications, the person with advancing dementia who does not require skilled nursing care but requires constant supervision and assistance for basic safety. These are the situations where Medicare’s coverage ends and the household is left with the full cost of ongoing care — exactly the situation that long-term care insurance exists to fund.
For households that have been planning around the assumption that Medicare would handle long-term care costs, discovering the coverage gap can create urgency about protecting retirement assets before a care event arrives. Our resources on how much long-term care insurance you need and how much long-term care insurance costs provide the practical framework for sizing coverage appropriately and evaluating whether the premium is justified by the protection it creates against the exposure Medicare leaves uncovered. Our resource on long-term care insurance services covers our complete independent LTC brokerage approach across more than 100 A-rated carriers.
Hybrid LTC Designs — Coverage That Works Alongside Medicare
For households that find the “use it or lose it” aspect of traditional long-term care insurance a barrier to planning, hybrid life insurance with LTC benefits and annuity-based LTC designs offer structures where the premium creates value regardless of whether care is ever needed — either through a death benefit that passes to heirs if care never occurs, or through contract value that remains in the annuity if the LTC benefit is never triggered. These hybrid designs coordinate directly with Medicare by covering the custodial care gap that Medicare cannot address, activating when the insured meets the standard 7702B benefit triggers (inability to perform 2 of 6 ADLs or severe cognitive impairment) that define genuine long-term care need.
Our resources on hybrid long-term care strategies, hybrid life insurance with long-term care benefits, affordable hybrid long-term care policies, and annuity with long-term care benefits cover these designs in detail. The coordination with Medicare is straightforward in practice: Medicare handles acute medical care during hospitalizations and qualified short-term skilled nursing recovery; long-term care insurance handles the custodial care that Medicare cannot fund after the acute recovery phase ends or when a chronic care need exists without an acute medical trigger at all. These two programs are complementary rather than overlapping — which is exactly why both have an important role in a complete retirement protection plan.
Close the Long-Term Care Gap Medicare Leaves
We compare traditional LTC, hybrid life/LTC, and annuity-based LTC designs — and show you exactly how each protects against the costs Medicare cannot cover, at your age, health profile, and budget.
Request My LTC Coverage ReviewRelated Medicare and Long-Term Care Resources
Explore the complete picture of Medicare’s limitations and the long-term care planning strategies that fill the gap.
Financial Protection Essentials
Connect Medicare’s coverage limitations to a complete retirement protection plan — including LTC insurance, Medicare supplement options, and annuity-based care funding strategies.
Questions now? Call 800-533-5969
Frequently Asked Questions: Does Medicare Cover Long-Term Care?
Does Medicare pay for nursing home care?
Medicare pays for short-term skilled nursing facility care only — not long-term custodial nursing home care. Specifically, Medicare Part A covers up to 100 days of skilled nursing facility care per benefit period following a qualifying 3-day inpatient hospital stay, for a condition related to the hospitalizing diagnosis, when daily skilled care remains medically necessary. Days 1 through 20 are fully covered. Days 21 through 100 require a copayment of $209.50 per day in 2025. After Day 100, Medicare covers nothing. Custodial nursing home care — the ongoing personal assistance with Activities of Daily Living that most people need in a nursing home long term — is not covered by Medicare at any point regardless of how long the person has been there.
Does Medicare cover assisted living?
No. Assisted living is not a Medicare-covered care setting under any circumstances. Medicare does not pay for room, board, personal care, or assistance with Activities of Daily Living in an assisted living facility. If a person in an assisted living facility has a specific skilled care need — a physician-ordered home health visit for wound care, for example — Medicare might cover that specific skilled visit, but not the assisted living cost itself. The full cost of assisted living — which can range from approximately $4,000 to $8,000 or more per month depending on location and level of care — is private pay and must be funded from personal savings, long-term care insurance, or Medicaid in states where home and community-based waivers cover assisted living for qualifying individuals.
Does Medicare cover home health care for long-term needs?
Medicare covers limited home health services — but only for intermittent, part-time skilled care ordered by a physician, for a specific medical condition, when the patient is homebound. Medicare home health is not designed for ongoing daily personal care or full-time home health aide services. When the skilled component ends — when therapy goals are achieved or the physician determines skilled care is no longer medically necessary — the Medicare home health benefit ends entirely, including any accompanying aide services. The person who needs 6 to 8 hours per day of home care assistance for ongoing functional or cognitive limitations will not find that level of support within Medicare’s home health benefit.
What is the difference between skilled care and custodial care for Medicare purposes?
Skilled care in Medicare’s framework means care requiring licensed medical professionals — nurses, physical therapists, occupational therapists — for medically necessary treatment such as wound care, IV therapy, complex medication management, or intensive rehabilitation. Custodial care means ongoing personal assistance with Activities of Daily Living — bathing, dressing, eating, toileting, transferring, and continence — that does not require licensed medical professional skills on a daily basis. Medicare covers skilled care (with time and eligibility limits). Medicare does not cover custodial care under any conditions. Since most long-term care need is custodial in nature — ongoing personal assistance with daily functioning — Medicare does not cover most of what people think of as “long-term care.”
Does Medicare Advantage cover long-term custodial care?
No. Medicare Advantage plans are required to provide the same coverage as Original Medicare Parts A and B — which does not include custodial long-term care. Some Medicare Advantage plans, particularly Chronic Special Needs Plans and plans with SSBCI benefits, may provide limited supplemental in-home supports, transportation assistance, or meal delivery for chronically ill members. These supplemental benefits can reduce friction for specific health situations but are not a substitute for ongoing custodial care funding. The custodial care gap — the cost of daily personal assistance with Activities of Daily Living — is not covered by Medicare Advantage under any standard plan design.
What is the observation status trap in Medicare?
Observation status is a Medicare classification that designates a hospital patient as an outpatient — rather than a formally admitted inpatient — even when the patient is physically in a hospital bed for multiple nights. Days spent under observation status do not count toward the 3-consecutive-inpatient-day qualifying requirement for Medicare’s skilled nursing facility benefit. A patient who spends multiple nights in the hospital but only 2 days as a formally admitted inpatient does not qualify for Medicare SNF coverage and will be billed for the entire subsequent SNF stay as private pay. Patients and families should ask their hospital care team explicitly: “Am I admitted as an inpatient or am I under observation status?” The answer determines whether the 3-day qualifying requirement can be met.
How does long-term care insurance fill the gap that Medicare leaves?
Long-term care insurance covers the custodial care that Medicare categorically excludes — ongoing assistance with Activities of Daily Living at home, in assisted living, in memory care, in adult day programs, and in skilled nursing facilities beyond Medicare’s 100-day limit. LTC insurance benefits are typically triggered when the insured is unable to perform 2 or more of 6 Activities of Daily Living for a period expected to last at least 90 days, or when severe cognitive impairment requires substantial supervision — the same functional and cognitive standards that define genuine long-term dependence. These triggers align with real care need rather than with what a physician must certify as medically necessary skilled treatment, making LTC insurance the appropriate funding mechanism for the care that Medicare cannot address.
About the Author:
Tonia Pettitt, CMIP©, (NPN 14374308), is a seasoned Medicare specialist with more than 40 years of hands-on experience guiding individuals and families through the complexities of Medicare planning. As a senior advisor with the nationally licensed independent agency Diversified Insurance Brokers, Tonia provides clear, dependable guidance across all areas of Medicare—including Medicare Advantage, Medicare Supplement (Medigap), and Part D prescription coverage. Leveraging active contracts with dozens of highly rated insurance carriers, she helps clients compare options objectively and secure the most suitable coverage for their health and budget.
Known for her patient, education-first approach, Tonia has built a reputation as a trusted resource for retirees seeking reliable, unbiased Medicare support. With four decades of experience across evolving Medicare laws, carrier changes, and plan structures, she brings unmatched insight to every client conversation—ensuring clients feel confident, protected, and fully prepared for each stage of their retirement healthcare journey.
Explore More Medicare Options: Browse our complete guide to How Does Medicare Work? — covering Medicare Parts A, B, C & D explained — coverage, costs & how it all fits together.
Explore More Long Term Care Insurance Options: Browse our complete guide to Tax, Medicare & Special Situations — covering tax advantages, Medicare vs LTC, seniors, couples, diabetics & age-specific coverage from top carriers.
Last Reviewed: May 25, 2026 |
Reviewed by: Tonia Pettitt, CMIP©
Medicare Specialist, Diversified Insurance Brokers, Inc. | NPN: 14374308 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Fact Checked by: Jason Stolz, CLTC, CRPC, DIA, CAA
Chief Underwriter, Diversified Insurance Brokers, Inc. | NPN: 20471358 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Editorial Standards: Diversified Insurance Brokers maintains rigorous editorial standards to ensure accuracy, clarity, and independence in all content. Learn more about our editorial standards and commitment to transparency.
