Self Insured Long Term Care
Self Insured Long Term Care

Jason Stolz CLTC, CRPC, DIA, CAA
Self-insured long term care is one of the most common retirement planning postures in America — and one of the most misunderstood. For many households, it is not a deliberate strategy built on careful analysis of their financial capacity to absorb extended care costs. It is a default: the outcome of never having formally addressed long term care risk, combined with a sense that “we have enough assets” or “we’ll figure it out when the time comes.” True self-insurance — retaining a risk because you have analyzed it, priced it, and determined that your financial resources are sufficient to absorb worst-case outcomes without compromising your household’s financial plan — is a legitimate approach for a relatively small subset of retirees with very substantial, very liquid assets far exceeding any realistic care cost scenario. For most households, what is described as self-insuring is actually uninsured exposure to a large, unpredictable, inflation-sensitive liability that can last years and arrive at the worst possible moment in a retirement portfolio’s lifecycle.
At Diversified Insurance Brokers, we help households make this decision with accurate cost data, realistic scenario modeling, and a clear-eyed comparison of what self-funding actually costs versus what LTC insurance or hybrid strategies actually provide. The decision to self-fund long term care risk should be made after examining the numbers — not by assumption. Our resource on whether long term care insurance is worth it covers the foundational value framework, and our resource on long term care planning strategies covers the full strategic context within which the self-fund vs. transfer decision sits.
Protect Retirement Assets From Long-Term Care Risk
Compare traditional LTC, hybrid, and single-pay options tailored to your goals and budget — see what the alternatives to self-funding actually cost and deliver.
Request Your LTC QuoteWhat Self-Insured Long Term Care Actually Means
The term “self-insured” implies intentionality and financial sophistication — and for corporations and governments that formally self-insure specific risks, it does represent a deliberate strategy backed by actuarial analysis, reserve requirements, and formal risk management programs. When individual retirees describe themselves as “self-insured” for long term care, the reality is usually quite different. Insurance works by pooling risk across a large group of people: premiums collected from thousands of policyholders fund the care costs of the fraction who experience significant claims, creating leverage that allows any individual to access far more in benefits than they contributed in premiums. When an individual “self-insures,” they receive no leverage and bear the entire cost of any claim from their own resources — with no upper bound on exposure and no guarantee that the claim will arrive at a financially convenient time.
The distinction matters enormously because long term care is not a fixed, predictable expense like a mortgage or a car payment. It is an open-ended liability with a duration that can range from a few months to a decade or more, a cost that increases with medical inflation at rates that historically exceed general consumer inflation, and a timing that is entirely outside the individual’s control. A household that has accumulated $500,000 in retirement savings might reasonably believe it can absorb long term care costs. But a three-year memory care journey at $7,000 per month in a metropolitan area — entirely within the range of current costs — consumes $252,000 in care costs alone. After taxes on the retirement account withdrawals funding those costs and the investment returns foregone on the liquidated assets, the financial damage is substantially larger. Our resource on the cost of long term care by state provides the regional cost benchmarks that should anchor any realistic self-funding analysis.
Comparing Approaches: Self-Funding vs. LTC Coverage Options
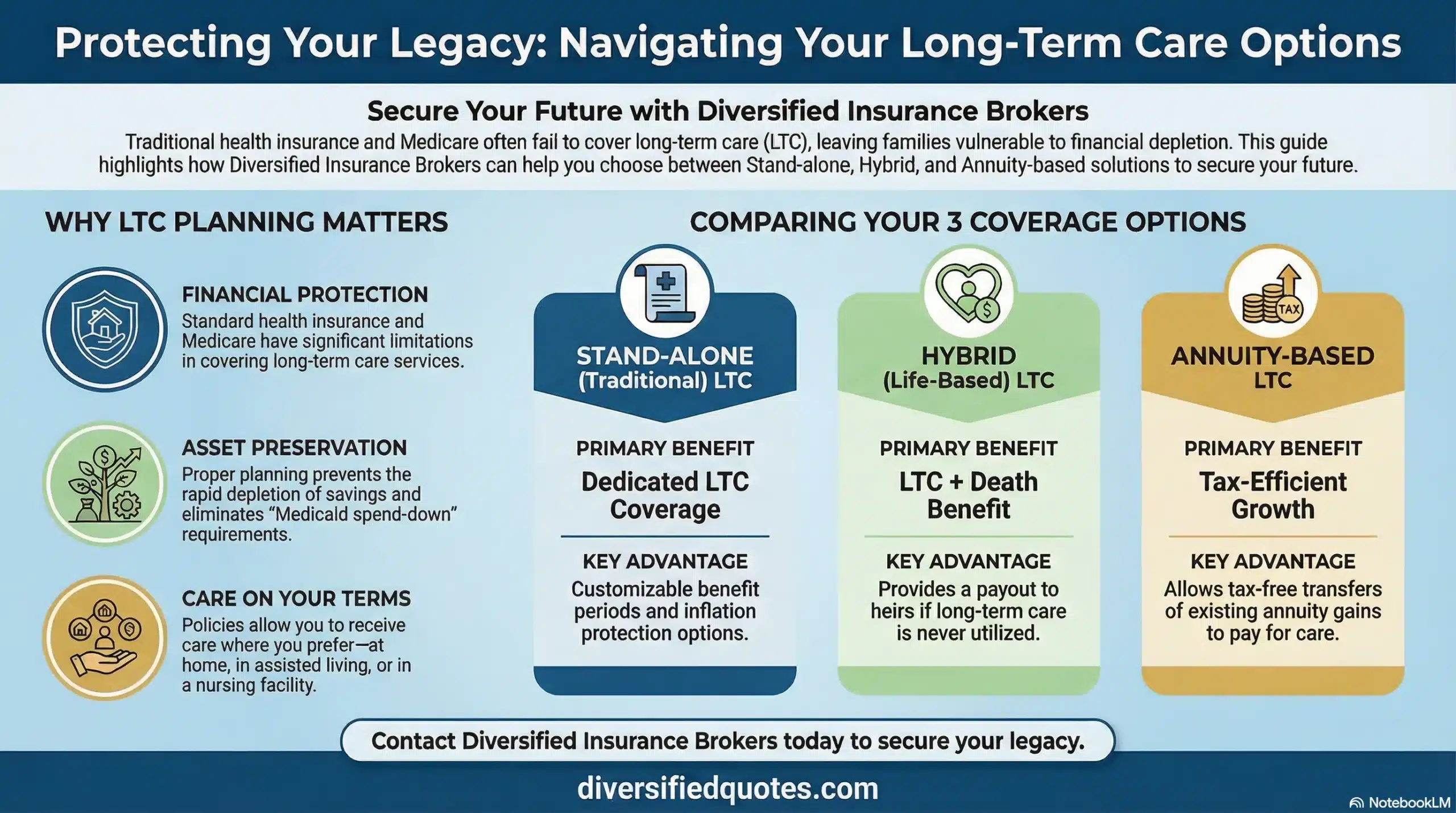
The most useful way to evaluate whether self-funding long term care risk is appropriate for a specific household is to compare it directly against the available transfer alternatives — not in abstract terms, but on the specific dimensions that determine real-world financial performance. The table below maps the five primary approaches across the key dimensions that matter most in this comparison.
Long-Term Care Risk Approaches: Self-Funding vs. Insurance and Hybrid Options
| Approach | Cost Structure | Coverage When Care Needed | Value If Care Not Needed | Best For |
|---|---|---|---|---|
| Pure Self-Funding | Personal assets; no upper limit on exposure; no premium | Whatever assets remain; no leverage; no guaranteed benefit pool | Full asset retention if care never needed | Very high net worth; liquid reserves far exceeding worst-case scenarios |
| Traditional LTC Insurance | Ongoing premiums (possible rate adjustments); tax-advantaged | Defined monthly benefit pool with high leverage; generally tax-free benefits | No residual value to heirs (traditional); risk transferred during coverage years | Maximum LTC leverage per dollar; healthy buyers in 50s–early 60s |
| Hybrid Life + LTC | Single premium (repositioned asset) or limited pay | Death benefit accelerated for care; defined monthly maximum | Full death benefit to heirs if care not needed; “value either way” | Legacy-focused buyers; “use it or lose it” objection to traditional LTC |
| Hybrid Annuity + LTC | Single premium; often funded via 1035 exchange from existing annuity | Annuity value multiplied 2–3x for qualifying care; defined benefit period | Account value retained; available for income or legacy | Asset repositioners; households with low-yield or idle savings to redeploy |
| Partial Transfer + Self-Fund | Insurance premium covers catastrophic risk; self-fund covers early/minor needs | Insurance activates for extended care after elimination period; self-fund covers the gap | Self-funded reserves remain; insurance risk not activated | Budget-conscious households; moderate net worth; willing to absorb short-term costs |
The self-funding approach’s apparent advantage — no premium, full asset retention if care is never needed — comes with a corresponding disadvantage: no leverage and unlimited exposure. The insurance and hybrid approaches trade a defined cost (premium or repositioned premium) for a defined benefit pool that substantially exceeds what could be funded with the same premium amount. This leverage is the economic reason insurance exists: it allows a predictable, manageable cost to create protection against an unpredictable, potentially catastrophic expense. Our resource on how much long term care insurance you need covers the benefit-sizing methodology that determines whether an insurance approach provides adequate coverage for a specific household’s exposure.
The Mathematics of Self-Funding Long Term Care
The financial mathematics of self-funding long term care deserve explicit examination, because the numbers look different in practice than in the abstract. The most common self-funding rationalization sounds like this: “We have $800,000 in retirement savings. If care costs $100,000 per year, we can handle three to five years.” This calculation has several hidden problems that the initial math obscures.
The first problem is gross versus net costs. Most retirement savings are in tax-deferred accounts — traditional IRAs, 401(k)s, and similar accounts where withdrawals are taxable as ordinary income. To net $100,000 in care costs from a traditional IRA, the account owner may need to withdraw $130,000 to $140,000 before taxes, depending on their marginal bracket. In a high-care-cost year, this elevated income may also push the account holder into a higher marginal bracket, push Social Security income over a higher taxation threshold, and trigger Medicare premium surcharges (IRMAA) for the following two years. The actual cost of a $100,000 care year, measured in total economic impact on the household, may be significantly higher than the care cost alone.
The second problem is the sequence of returns risk. Long term care needs do not arrive on a predictable schedule. A household that experiences a major care event during a market downturn — which is exactly when financially stressed households are most vulnerable — faces compounding damage: they are forced to liquidate retirement assets at depressed prices to fund ongoing care costs, permanently reducing the portfolio’s future recovery capacity. A $300,000 care expenditure from a portfolio that has dropped 25 percent in value forces the liquidation of a larger percentage of remaining shares than the same expenditure from a portfolio at full value — and those shares are unavailable to participate in the eventual recovery. Our resources on guaranteed income at age 65 and guaranteed income at age 70 cover how guaranteed income strategies can protect against this sequence-of-returns vulnerability in retirement portfolios.
The third problem is duration uncertainty. Medical literature on care duration is sobering: while average care durations are often cited in the two-to-four-year range, averages mask the distribution. A significant minority of care journeys last six, eight, or more than ten years — particularly for progressive cognitive conditions like Alzheimer’s and Parkinson’s, which do not resolve and which typically require increasingly intensive care settings as the condition advances. A household budgeting for three to five years of care may be fully protected under one scenario and catastrophically underprotected under another. Insurance manages this distribution risk by pooling it; self-funding concentrates it entirely on the individual household without any pooling benefit.
Why Medicare Does Not Fill the Self-Funding Gap
One of the most persistent and consequential misunderstandings in retirement planning is the belief that Medicare will cover long term care costs if they arise. Medicare is a medical insurance program designed to cover acute medical care — hospital stays, physician services, skilled nursing care following a qualifying hospitalization (typically for up to 100 days under specific conditions), and rehabilitative services. It explicitly does not cover custodial care: the ongoing, day-to-day assistance with activities of daily living that constitutes the vast majority of long term care spending — help with bathing, dressing, transferring, toileting, and eating, plus cognitive supervision for dementia-related conditions.
The distinction between skilled care (covered by Medicare for limited periods) and custodial care (not covered by Medicare) is the coverage gap that long term care insurance is specifically designed to fill. A household that relies on Medicare as a backstop for long term care is relying on coverage that does not exist for the most common and most expensive care scenarios. Our resource on whether Medicare covers nursing home care and our related resource on whether Medicare covers long term care cover the specific Medicare coverage rules and the custodial care exclusion in detail. Understanding this exclusion before deciding to self-fund is not optional — it is the foundational fact that changes the self-funding math for most households.
The Surviving Spouse Vulnerability
For married couples, the self-funding approach to long term care carries a specific and serious risk that single individuals do not face in the same way: the surviving spouse vulnerability. When one spouse experiences a major care event and the household’s assets are depleted to fund that care, the surviving spouse — who may need to live on those same assets for another decade or more — inherits a significantly reduced financial position at exactly the moment when they are also dealing with grief, logistical demands, and potentially declining health of their own. The care costs of the first spouse can consume a substantial portion of the joint retirement assets that were supposed to support two lifetimes, leaving the surviving spouse with inadequate resources for their remaining years.
This vulnerability is one of the primary reasons that couple-focused LTC planning tools exist. Shared-care designs allow either spouse to access a combined benefit pool, rather than each spouse being limited to their own isolated benefit. Our resources on long term care insurance with shared benefits and long term care insurance with shared spousal benefits cover how these designs protect the household from the asymmetric care-cost scenario that most damages married couples’ financial plans. The surviving spouse’s financial security is one of the most compelling arguments against pure self-funding for married couples, and it is one of the arguments that most consistently moves households toward a coverage decision when it is modeled explicitly rather than assumed away.
Traditional LTC Insurance: How Leverage Works
Traditional long term care insurance creates economic leverage that self-funding cannot replicate. A healthy 58-year-old might pay $2,500 annually for a traditional LTC policy providing a $6,000 monthly benefit with a three-year benefit period and three percent compound inflation. The total benefit pool at policy issue is approximately $216,000. After ten years of $2,500 annual premiums and three percent compound benefit growth, the same pool has grown to approximately $290,000 — funded by $25,000 in total premiums. If a claim begins at that point and continues for three years, the policy pays approximately $290,000 in benefits. The leverage ratio — benefits received relative to premiums paid — is approximately 11-to-1.
No self-funded portfolio produces this kind of leverage for a specific, contingent expense. Self-funding requires dollar-for-dollar accumulation of the full care cost, plus the tax gross-up needed to net the care cost from taxable account withdrawals. The leverage differential between traditional LTC insurance and self-funding is the economic reason that LTC insurance exists — it converts a series of manageable premium payments into access to a much larger benefit pool that would require decades of additional accumulation to replicate through self-funding. Our resource on whether you should buy long term care insurance covers the value proposition at different net worth levels, and our resource on how to qualify for long term care insurance covers the underwriting requirements that determine eligibility at different ages and health profiles.
Hybrid Options: Repositioning Assets Rather Than Paying Premiums
For households whose primary objection to traditional LTC insurance is the “use it or lose it” concern — the possibility that premiums are paid for decades without ever triggering a benefit — hybrid life/LTC and annuity+LTC designs address that objection directly by providing value regardless of whether care is ever needed. These designs reposition an existing asset into a structure that creates care leverage when care is needed and death benefit or account value when care is not needed.
Hybrid life+LTC designs pair a life insurance death benefit with LTC accelerated benefits. If care is never needed, the full death benefit passes to heirs. If care is needed, the death benefit is drawn down to fund care, with any remaining death benefit passing at death. The household’s premium investment produces value in both scenarios — LTC coverage during life and a legacy benefit at death — eliminating the use-it-or-lose-it objection entirely. Our resource on hybrid life insurance with long term care benefits covers these designs in detail, and our broader resource on hybrid long term care covers the full landscape of hybrid LTC product categories.
Hybrid annuity+LTC designs work similarly for households that want to reposition existing savings — low-yield CDs, money market accounts, or older non-qualified annuities — into a structure that creates LTC leverage without requiring new cash contributions. Our resource on fixed annuity with long term care benefits covers this design, and our resource on single-pay long term care insurance covers the broader single-premium LTC planning category. For households wanting to compare all available options, our resource on how to choose the right long term care insurance policy covers the full selection framework across traditional, hybrid, and single-pay designs.
The Medicaid Backstop: Why It Is Not a Comfortable Strategy
Some households with moderate assets default to self-funding with the implicit assumption that Medicaid will provide coverage if their assets are eventually exhausted. Medicaid does provide long term care coverage — but only after the household has met the program’s means-testing requirements, which generally require spending down assets to very low levels (typically $2,000 in countable assets for the individual requiring care, though spousal protection rules allow the community spouse to retain more). The path from a moderate retirement portfolio to Medicaid eligibility runs directly through asset depletion, which is precisely the outcome that LTC insurance is designed to prevent.
Additionally, Medicaid long term care coverage is available only through Medicaid-contracted providers and facilities, which limits care choices significantly compared to what private-pay or insurance-funded residents can access. The ability to choose a care setting, select a facility, remain at home with private caregivers, or access memory care at a preferred provider is substantially curtailed for Medicaid beneficiaries. The “Medicaid backstop” strategy, when examined explicitly, means accepting asset depletion as an outcome and relinquishing care choice as a consequence. For households with meaningful retirement savings that they have worked decades to accumulate, this is rarely a satisfying outcome when it arrives. Our resource on LTC Partnership program reciprocity covers the state-level Partnership programs that allow qualifying LTC insurance policyholders to protect a corresponding dollar amount of assets from Medicaid spend-down when qualified benefits are exhausted — a meaningful alternative to pure Medicaid reliance for households considering how Medicaid eligibility interacts with their LTC planning.
Who Is Legitimately Well-Positioned to Self-Fund
Self-funding long term care is genuinely appropriate for a relatively small subset of retirees, and being clear about that subset is important for credible planning conversations. The household that is well-positioned to self-fund long term care has several specific characteristics working together, not just one of them in isolation.
The first characteristic is very substantial liquid, accessible assets — typically enough to absorb worst-case care cost scenarios (often modeled at five to eight years of full care, covering both spouses sequentially) without compromising the surviving spouse’s retirement income or legacy goals. For most metropolitan areas, a worst-case modeling number of $600,000 to $800,000 or more in care costs for a couple is not unreasonable, and this should be available from liquid assets beyond what is needed for income. Households for which this depletion scenario would be genuinely trivial relative to total wealth are legitimate candidates for self-funding.
The second characteristic is investment returns that reliably exceed care cost inflation on the dedicated care reserve, providing genuine self-insurance rather than just asset erosion. The third is the absence of a surviving spouse whose financial security depends on the assets being preserved. And the fourth is a genuine, modeled analysis of the self-funding math — not an assumption that self-funding is fine because “we have savings.” Many households that describe themselves as well-positioned to self-fund have never run the specific scenario analysis. Our resource on how long a solo 401(k) lasts in retirement provides portfolio longevity modeling context, and our resource on the investment risk calculator covers portfolio risk analysis that informs the self-funding adequacy question.
The Emotional and Family Dimensions of Self-Funding
The financial analysis of self-funded long term care addresses the balance sheet impact of care costs. It does not address the emotional, relational, and caregiving burden that self-funded care places on families — and that burden is substantial, often larger in practice than the financial burden that receives most of the planning attention.
When professional care is not funded by insurance, families often default to providing care informally — spouses providing care for each other, adult children taking time away from careers and families to provide care for parents, or siblings coordinating across geographic distance. Family caregiving is often described as one of the most stressful experiences in adult life, with documented health consequences for caregivers that include elevated rates of depression, anxiety, and physical illness. The availability of funded professional care — home health aides, care coordinators, adult day care services, assisted living — protects not just the care recipient’s quality of life, but the caregiver’s health and family relationships. Our resource on what adult day care is covers one of the care options that funded care enables and unfunded care often foregoes.
Insurance-funded care also enables better care decisions by removing the financial pressure that shapes decisions when care costs come entirely from personal assets. A family facing $8,000 per month in memory care costs from a depleting retirement portfolio makes care decisions under financial stress that families with funded care do not face. Choosing the right facility, deciding how long to maintain home care, determining when assisted living is needed — these decisions are made more clearly and more humanely when the financial constraint is removed by a benefit pool.
Model the Real Cost of Self-Funding vs. LTC Insurance
We’ll compare traditional LTC, hybrid, and single-pay options against the self-funding math for your specific asset level, location, and planning priorities.
Start Your LTC Planning ReviewRelated Pages: LTC Planning and Coverage Alternatives
Compare LTC coverage options, understand costs, and explore hybrid alternatives to self-funding.
Financial Protection Essentials
LTC cost calculators, tax advantage resources, coverage design guides, and retirement income planning tools.
Talk With an Advisor Today
Choose how you’d like to connect—call or message us, then book a time that works for you.
Schedule here:
calendly.com/jason-dibcompanies/diversified-quotes
Licensed in all 50 states • Fiduciary, family-owned since 1980
FAQs: Self-Insured Long-Term Care
What is the real difference between self-insuring and self-funding long term care?
True self-insurance, in the actuarial sense, means retaining a risk after formally analyzing it, pricing it, and determining that your financial capacity to absorb worst-case outcomes is adequate without compromising other financial goals. Insurance works by pooling risk across thousands of policyholders, creating leverage: a manageable premium contribution accesses a much larger benefit pool. When an individual “self-insures” long term care, they receive no pooling benefit and no leverage — they are simply retaining the risk entirely on their own balance sheet, without any upper bound on exposure and with no guarantee that a claim will arrive at a financially convenient time.
For most households, what is described as self-insuring is actually uninsured exposure to a large, open-ended liability. The distinction matters because the decision-making framework is different. True self-insurance requires running the specific worst-case care cost scenarios — duration of care, cost escalation with medical inflation, tax gross-up on retirement account withdrawals, sequence-of-returns impact if a claim arrives during a market decline — and confirming that those worst-case outcomes are genuinely manageable without compromising the household’s financial plan. Most households that describe themselves as self-insured have never run that analysis.
Why is paying for care out of pocket riskier than it appears?
Self-funding long term care appears manageable in the abstract — “we have $X in savings, care costs $Y per month, so we can cover Z years.” This calculation has several hidden costs that make the actual financial impact substantially larger than the care cost alone. The first is the tax gross-up: most retirement savings are in tax-deferred accounts where withdrawals are taxable as ordinary income. To net $100,000 in care costs, the household may need to withdraw $130,000 to $140,000 before taxes, depending on their bracket. In high-withdrawal years, this elevated income may trigger additional Medicare premium surcharges and Social Security taxation at higher thresholds.
The second hidden cost is the sequence-of-returns risk. Care events do not arrive on schedule, and if a major care event coincides with a market downturn, the household is forced to liquidate retirement assets at depressed prices to fund ongoing care costs. Those liquidated shares are unavailable to participate in the eventual recovery, permanently reducing the portfolio’s future value. The third hidden cost is duration uncertainty — care journeys for cognitive conditions can last a decade or more, far exceeding the two-to-four-year averages that many households use as their planning assumption. Insurance pools this duration risk across many policyholders; self-funding concentrates it entirely on one household without any pooling benefit.
Won’t Medicare cover long term care costs?
No. Medicare is a medical insurance program that does not cover custodial long term care — the ongoing daily assistance with activities of daily living that constitutes the vast majority of long term care spending. Medicare covers acute medical care: hospital stays, physician services, skilled nursing care following a qualifying hospitalization (for up to 100 days under specific conditions), and rehabilitative services. When care is needed for bathing, dressing, transferring, toileting, eating, or cognitive supervision — which is the profile of most care journeys — Medicare does not pay for it.
This is not a planning technicality or an obscure exception. It is the fundamental structural gap that long term care insurance was designed to address. Many retirees discover this gap for the first time when a parent requires care, at which point the discovery is too late to influence planning. The household that relies on Medicare as a long term care backstop is relying on coverage that does not exist for the most common and most expensive care scenarios. Planning decisions should account for this reality explicitly rather than assuming Medicare provides broader coverage than it does.
Is long term care insurance too expensive compared to self-funding?
Traditional long term care insurance typically delivers the highest LTC benefit leverage per premium dollar of any available approach — meaning the ratio of potential benefits to premiums paid is substantially higher than the ratio of benefits available to assets retained in a self-funded approach. A healthy buyer in their late 50s paying $2,500 to $4,000 annually for traditional LTC insurance creates access to a benefit pool of $200,000 to $400,000 or more, depending on benefit design and inflation provisions. No savings accumulation strategy produces this leverage for a specific contingent expense without decades of additional contribution and compounding.
The “too expensive” perception often reflects a comparison of the certain premium cost against the uncertain probability of using the benefit — rather than a comparison of the premium against the actual care cost exposure being transferred. The relevant comparison is not “LTC premium vs. zero” — it is “LTC premium vs. the full self-funding cost if care is needed,” measured in real dollars including the tax and sequence-of-returns costs described above. When the comparison is framed correctly, the insurance premium often represents an attractive cost for the protection it provides. Hybrid designs that return value to heirs if care is never needed address the use-it-or-lose-it concern for households for whom that is the primary objection.
What is the advantage of single-pay or hybrid LTC designs over traditional insurance?
Single-premium and hybrid LTC designs address two of the most common objections to traditional long term care insurance: the ongoing premium commitment and the use-it-or-lose-it concern. A single-premium design is funded with a lump sum — often repositioned from an existing low-yield CD, money market account, or older non-qualified annuity — rather than requiring ongoing annual premium payments. The premium amount is fixed at purchase and never increases. This eliminates premium uncertainty and converts a passive savings holding into active protection with LTC leverage.
Hybrid designs — life insurance + LTC or annuity + LTC — go further by ensuring that the premium investment produces value in both scenarios. In a hybrid life+LTC design, if care is never needed, the death benefit passes to heirs income-tax-free. If care is needed, the death benefit is drawn down to fund care costs. In a hybrid annuity+LTC design, if care is never needed, the annuity value continues as a retirement asset. If care is needed, the annuity value is multiplied for care expenses. Both hybrid approaches eliminate the use-it-or-lose-it objection by providing guaranteed value regardless of whether the LTC benefit activates.
Can I get LTC coverage if I have existing health conditions?
Eligibility for long term care insurance varies by carrier, health condition, severity, and stability. Traditional LTC underwriting is generally more comprehensive and more restrictive than the simplified underwriting used by most hybrid designs. For buyers with health conditions that create uncertainty in traditional LTC underwriting, hybrid life+LTC and annuity+LTC designs often have more accessible underwriting standards while still providing meaningful care protection. The right approach depends on the specific health history and which carriers have underwriting guidelines compatible with that history.
The most important practical point about health and LTC underwriting is timing: underwriting becomes more restrictive, premiums increase, and coverage options narrow as age and health conditions progress. A health condition that is manageable in an underwriting context at 58 may be a disqualifying factor at 68. Planning earlier — when health is better and underwriting options are broadest — consistently produces better coverage outcomes than planning after health changes have occurred. Our resource on how to qualify for long term care insurance covers the underwriting framework in detail, and we pre-screen applicant profiles across multiple carriers to identify the best available options for each specific health situation.
What if I never need long term care?
Under a pure self-funding approach, never needing long term care is the best outcome — assets remain intact and available for retirement income and legacy. Under traditional LTC insurance, never needing care means the premium investment was used to transfer risk during the years of coverage, which is the same economic function as homeowner’s insurance that never pays a claim. The premiums purchased protection; the fact that protection was not needed is a good outcome, not a loss.
For households whose primary concern is the use-it-or-lose-it dynamic, hybrid designs provide the “value either way” structure that addresses this concern directly. Hybrid life+LTC provides a guaranteed death benefit to heirs if LTC benefits are never accessed. Hybrid annuity+LTC retains account value for the policyholder’s retirement income or legacy if care is never needed. These designs are specifically structured so that the premium investment produces certain, defined value in both the care-needed and care-not-needed scenarios — making the coverage decision feel more like asset repositioning than premium payment.
About the Author:
Jason Stolz, CLTC, CRPC, DIA, CAA and Chief Underwriter at Diversified Insurance Brokers (NPN 20471358), is a senior insurance and retirement professional with more than 25 years of real-world experience helping individuals, families, and business owners protect their income, assets, and long-term financial stability. As a long-time partner of the nationally licensed independent agency Diversified Insurance Brokers, Jason provides trusted guidance across multiple specialties—including fixed and indexed annuities, long-term care planning, personal and business disability insurance, life insurance solutions, Group Health, Travel Medical and Evacuation Insurance, and short-term health coverage. Diversified Insurance Brokers maintains active contracts with over 100 highly rated insurance carriers, ensuring clients have access to a broad and competitive marketplace.
His practical, education-first approach has earned recognition in publications such as VoyageATL, and contributions from his agency featured in Kiplinger and GoBankingRates— highlighting his commitment to financial clarity and client-focused planning. Drawing on deep product knowledge and years of hands-on field experience, Jason helps clients evaluate carriers, compare strategies, and build retirement and protection plans that are both secure and cost-efficient. Visitors who want to explore current annuity rates and compare options across multiple insurers can also use this annuity quote and comparison tool.
Explore More Long Term Care Insurance Options: Browse our complete guide to LTC Insurance Costs, Rates & Planning — covering how much it costs, best rates, calculators, planning strategies & is it worth it from top carriers.
Last Reviewed: May 21, 2026 |
Reviewed by: Jason Stolz, CLTC, CRPC, DIA, CAA
Chief Underwriter, Diversified Insurance Brokers, Inc. | NPN: 20471358 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Fact Checked by: Tonia Pettitt, CMIP©
Medicare Specialist, Diversified Insurance Brokers, Inc. | NPN: 14374308 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Editorial Standards: Diversified Insurance Brokers maintains rigorous editorial standards to ensure accuracy, clarity, and independence in all content. Learn more about our editorial standards and commitment to transparency.
