What is a Skilled Nursing Facility
What is a Skilled Nursing Facility

Jason Stolz CLTC, CRPC, DIA, CAA
A skilled nursing facility (SNF) is the highest-acuity residential care setting in the long-term care spectrum — a licensed, Medicare-certified medical environment that provides 24-hour nursing oversight, rehabilitation therapy, physician supervision, medication management, and clinical monitoring for individuals whose care needs exceed what can safely be delivered at home or in assisted living. Skilled nursing facilities sit at the top of the care intensity ladder, and they represent the most expensive long-term care setting by a substantial margin. Medicare Part A covers SNF care for up to 100 days per benefit period — but the coverage structure has three distinct phases: the first 20 days are covered in full, days 21 through 100 require a daily coinsurance payment from the patient, and from day 101 onward Medicare pays nothing. The daily coinsurance for days 21–100 is updated by CMS each fall — verify the current year’s rate at Medicare.gov. Understanding these three phases is the foundation of understanding why long-term care planning matters so much for families who may face extended SNF stays. Medicare’s coverage is time-limited, medically conditional, and stops entirely at day 100 of any benefit period. Beyond that threshold, the financial exposure falls entirely to the patient and their family unless another funding source — long-term care insurance, Medicaid, or designated retirement assets — is in place.
Most families first encounter skilled nursing facilities as a short-term post-hospitalization destination. A joint replacement, a stroke, a cardiac event, a major surgery — any acute medical event requiring 24-hour nursing oversight beyond what a hospital inpatient stay provides may result in discharge to a skilled nursing facility for a rehabilitation period before returning home. This short-term rehab scenario is the most common entry point, and many families complete that stay and return home without developing a longer-term relationship with the SNF system. The planning risk lies in what happens when that short-term stay either extends beyond Medicare’s covered period, or when a subsequent care need requires long-term skilled nursing care because the individual’s medical complexity or functional limitations make sustained home living unsafe. In those scenarios, costs accumulate at several thousand dollars per month — and without a funding plan, those costs are drawn directly from retirement savings. Our long-term care insurance services overview covers how LTC policies are specifically structured to address this funding gap, and our protect your nest egg resource covers the broader asset protection strategy that SNF planning sits within.
The distinction between skilled care and custodial care is the most consequential concept in SNF financial planning — and the one most often misunderstood. Medicare pays for skilled care: medically necessary services that require the training and judgment of licensed clinical professionals. Medicare does not pay for custodial care: daily living assistance (bathing, dressing, eating, mobility, toileting, continence) that can be delivered safely by non-licensed caregivers. The moment a SNF patient no longer needs skilled nursing or therapy services on a daily basis — even if they still need substantial personal care assistance — Medicare coverage stops, regardless of how many benefit days remain. This transition from skilled to custodial status is the most common trigger for unexpected SNF costs for families relying on Medicare as their primary funding source. Understanding whether Medicare covers long-term care and how Medicare differs from long-term care insurance are both essential pre-planning frameworks this page develops in detail.
Build a Skilled Nursing Cost Protection Plan
We help families evaluate LTC insurance, hybrid LTC strategies, and annuity-based funding options designed to help cover skilled nursing facility costs beyond Medicare’s limits. Independent comparison, no obligation.
SNF vs. Nursing Home vs. Assisted Living — Understanding the Care Spectrum
The terminology of senior care settings is imprecise in common usage, and that imprecision creates planning errors when families make coverage and funding assumptions based on incorrect category matching. Understanding the distinctions between skilled nursing facilities, nursing homes, assisted living facilities, and memory care units is essential before any informed long-term care discussion can occur.
A skilled nursing facility in the regulatory sense is a Medicare-certified and Medicaid-certified care facility that provides medically necessary services under physician supervision. The “skilled” designation specifically refers to the level of clinical services provided — registered nurses, licensed therapists, and other licensed clinical professionals delivering care that requires their specific training and judgment. Not every building labeled a “nursing home” is a certified SNF for Medicare billing purposes. Families need to confirm Medicare certification status before assuming Medicare will cover care in a specific facility.
Nursing homes in general usage typically refer to long-term residential care for individuals who cannot live independently and require ongoing personal care and supervision. Many nursing homes operate both a Medicare-certified skilled unit (for short-term rehab and acute care) and a long-term custodial wing (for residents who do not meet skilled care criteria). The coexistence of these two service levels within one building is a common source of confusion about what Medicare will and won’t pay for at any given time during a stay.
Assisted living facilities represent a substantially lower acuity level — residential settings that provide meals, housekeeping, personal care assistance, and limited supervision without continuous medical oversight. Memory care units within assisted living settings provide specialized environments for individuals with dementia — secure layouts, specialized programming, and trained staff — without necessarily providing the level of medical oversight a SNF delivers. The table below summarizes the key distinctions across care settings.
| Feature | Skilled Nursing Facility (SNF) | Assisted Living | Memory Care Unit | In-Home Care |
|---|---|---|---|---|
| Nursing Oversight | 24/7 licensed nursing | Limited; varies by state | Some; dementia-focused staff | Provider-dependent |
| Medicare Certification | Required for Medicare billing | Not Medicare-certified | Not Medicare-certified | Home health agencies may be |
| Rehab Therapy (PT/OT/Speech) | On-site daily | Limited; often off-site | Minimal | Home health may include PT/OT |
| ADL Assistance | Full — CNAs on shift 24/7 | Full — aides available | Full — dementia-trained | Full — during scheduled hours |
| Relative Cost Level | Highest — see Genworth Cost of Care Survey | Moderate — roughly half of SNF rates | Moderate to high | Moderate (full-time equivalent) |
| Medicare Covers? | Up to 100 days/benefit period (conditions apply) | No | No | Limited skilled home health only |
| LTC Insurance Covers? | Yes — once benefit triggers met | Yes — once benefit triggers met | Yes — once benefit triggers met | Yes — once benefit triggers met |
For current cost benchmarks by care setting and region, see the annual Genworth Cost of Care Survey at genworth.com — updated each year and searchable by geographic market. For Medicare coverage amounts, see Medicare.gov.
What Services Skilled Nursing Facilities Provide
The service profile of a skilled nursing facility is governed both by Medicare and Medicaid certification requirements and by the clinical needs of the resident population. Understanding what a SNF provides — and what distinguishes it from lower-acuity settings — helps families evaluate whether a specific care situation requires SNF level care or whether a lower-cost setting can safely meet those needs.
Nursing care is the defining service. SNFs employ registered nurses (RNs) and licensed practical nurses (LPNs) who provide around-the-clock clinical oversight: medication administration, wound care management, catheter care, IV therapy, pain management, and clinical monitoring of chronic and acute conditions. Certified nursing assistants (CNAs) provide personal care support under nursing supervision — assisting with bathing, dressing, transfers, toileting, and meals. The nursing staff density in a SNF is meaningfully higher than in assisted living, which is the primary driver of the higher cost and the higher clinical capability.
Rehabilitation therapy is one of the most common reasons for SNF admission. Physical therapy addresses mobility, strength, balance, and functional movement — critical for recovery from orthopedic surgery, stroke, or fall-related injury. Occupational therapy addresses the ability to perform activities of daily living and adapts techniques to support maximum independence. Speech-language pathology addresses swallowing difficulties, communication changes, and cognitive rehabilitation. These three therapy disciplines work in a coordinated interdisciplinary team that includes the attending physician, nursing staff, and social workers. Most Medicare-covered SNF stays are admission-driven by the need for this rehabilitation support.
Clinical monitoring for complex conditions distinguishes a SNF from lower-acuity settings. Conditions including congestive heart failure, COPD, advanced diabetes, kidney disease, and sepsis recovery require ongoing clinical observation — vital sign monitoring, fluid balance tracking, laboratory value review, and medication adjustment based on real-time clinical status. These monitoring functions require licensed clinical staff and cannot be replicated in assisted living or home care settings at the same level of oversight. For individuals with multiple chronic conditions requiring daily clinical management, SNF care may be the only safe option even when the acute event that prompted admission has resolved.
Medicare SNF Coverage — The Three-Phase Structure
Medicare Part A covers skilled nursing facility care under specific eligibility requirements and for a limited time period with increasing cost-sharing over the benefit period. The structure has three distinct phases that apply regardless of the specific dollar amounts published in any given year.
| SNF Stay Phase | Medicare Coverage | Patient Responsibility | Planning Note |
|---|---|---|---|
| Days 1–20 | 100% (after Part A deductible for the benefit period) | $0 per day for SNF costs | Part A deductible applies per benefit period — see Medicare.gov for current amount |
| Days 21–100 | Partial — Medicare pays the balance above the daily coinsurance | Daily coinsurance — see Medicare.gov for current rate | CMS updates this rate annually; Medigap policies cover it to varying degrees |
| Day 101 and beyond | $0 — Medicare pays nothing | 100% of all SNF costs | This is where LTC insurance and Medicaid planning matter most |
| When skilled care ends (any day) | $0 — Medicare stops immediately | 100% of all costs from that point | Medicare covers skilled care only — custodial care is never covered |
CMS updates the Medicare Part A benefit amounts each fall, effective January 1 of the following year. For the current year’s SNF coinsurance rate, Part A deductible, and benefit period rules, always verify at Medicare.gov — these are the official, authoritative numbers. This page describes the coverage structure, which is stable year-to-year; the specific dollar amounts are indexed to healthcare inflation and change annually.
The 3-Day Hospital Stay Rule — The Qualification Requirement Most Families Miss
Medicare’s SNF coverage requires a qualifying inpatient hospital stay of at least three consecutive days (not counting the day of discharge) before admission to a skilled nursing facility. This seems straightforward but produces one of the most common and financially significant surprises families encounter in the Medicare system: the difference between inpatient status and observation status.
When a patient is admitted to a hospital, their status is either “inpatient” or “under observation.” Inpatient status counts toward the three-day qualifying stay requirement for Medicare SNF coverage. Observation status does not — even if the patient is physically present in the hospital for three or more days receiving care in a bed. A patient who spends several days in the hospital under observation status and is then discharged to a skilled nursing facility will find that Medicare does not cover the SNF stay because the qualifying inpatient requirement was not met. This distinction can produce very large unexpected expenses, and it is not always clearly communicated by hospital staff during admission. Families should ask directly and explicitly about their loved one’s admission status — inpatient or observation — and understand the downstream implications before discharge planning occurs. This is a structural rule that has not changed; what changes annually are only the associated dollar amounts.
The facility must also be a Medicare-certified SNF, and the care received at the SNF must be for a condition treated during the qualifying hospital stay. Understanding how Medicare works in detail — including these precise eligibility conditions — is foundational to understanding why private LTC insurance exists as a distinct and necessary coverage category for most families.
The Cost of Skilled Nursing Care — What to Expect and Where to Verify
Skilled nursing facility care is consistently the highest-cost setting in the long-term care spectrum. SNF rates nationally are tracked and published annually by Genworth Financial’s Cost of Care Survey, updated each year and searchable by state and local market at genworth.com. The survey is the industry-standard reference for cost benchmarking across all care settings. Because costs vary substantially by geographic region — with urban markets and coastal states frequently running 20%–50% above national medians — looking up local rates is more useful than relying on national averages for personal planning purposes.
The pattern that matters more than any specific number is the cost hierarchy: skilled nursing facilities are consistently the most expensive care setting, typically running roughly two to three times the cost of assisted living, and several times the cost of adult day care. The financial exposure from extended SNF care — anything beyond what Medicare covers — is open-ended and can run into the hundreds of thousands of dollars over multi-year stays. This is why protecting retirement funds from SNF costs specifically requires advance planning rather than an assumption that Medicare or savings will be sufficient.
Short-Term Rehab vs. Long-Term Skilled Nursing Care — The Critical Distinction
Many families who encounter a SNF through a post-acute hospitalization experience assume that all SNF stays are temporary rehabilitation episodes with a return home as the expected outcome. This is true in many cases — a large proportion of Medicare-covered SNF stays are short-term rehab following orthopedic surgery, cardiac events, or pneumonia, and the majority of patients return home within 30–60 days. The planning challenge emerges in the cases that don’t follow this pattern.
Long-term skilled nursing care occurs when an individual’s medical complexity, daily living dependencies, or safety requirements make sustained home living unsafe or impossible even with substantial in-home support. This can occur as a direct result of the acute event that triggered hospitalization, or it can emerge gradually as a chronic condition progresses to the point where clinical management requires constant licensed oversight. For families who have not planned for this scenario — either through LTC insurance or retirement savings specifically designated for care costs — the transition from “this is temporary” to “this is now the plan” arrives without financial preparation and with rapidly mounting costs that Medicare’s 100-day limit cannot address.
How Long-Term Care Insurance Covers Skilled Nursing Facilities
Long-term care insurance is specifically designed to cover the care costs that Medicare does not — including the daily expenses of skilled nursing facility care from day one through the policy’s benefit period, without the 100-day limit, the 3-day hospital stay requirement, or the skilled care-only restriction. Most modern LTC insurance policies cover SNF care once the policy’s benefit eligibility triggers are met: the insured needs substantial assistance with at least two of six activities of daily living or has a qualifying cognitive impairment requiring substantial supervision. Once eligible, the policy reimburses actual SNF costs up to the daily or monthly benefit limit stated in the policy, regardless of what Medicare does or doesn’t cover.
Evaluating how to qualify for long-term care insurance while in good health — and before a care need develops — is the primary timing consideration in LTC planning. For couples specifically, LTC insurance with shared spousal benefits and shared care riders provide flexible benefit pool designs that address the household’s combined SNF cost risk more efficiently than two separate individual policies. Our independent LTC broker resource covers how to compare policies across carriers to find coverage that fits your specific situation.
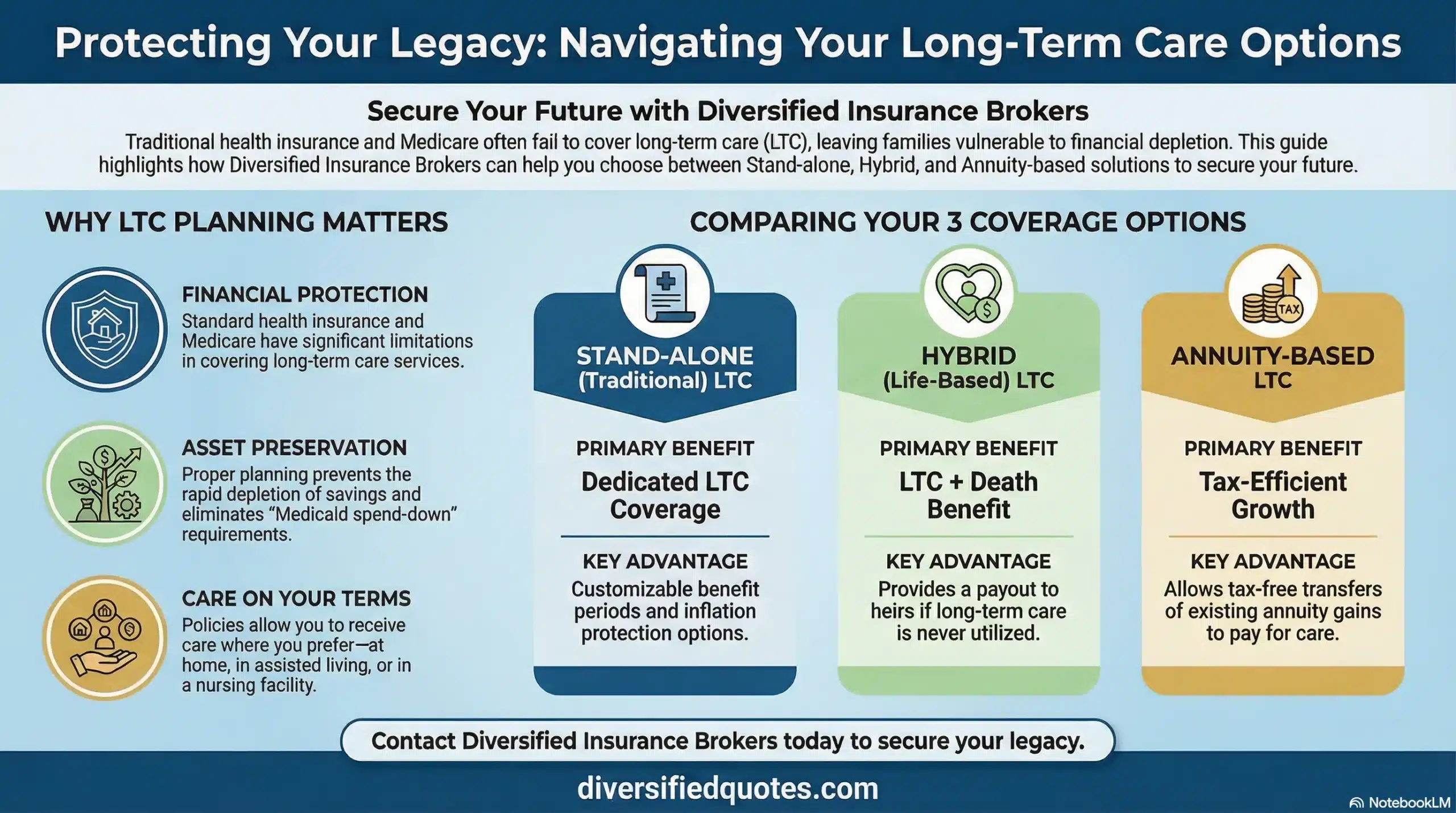
Several specialized LTC coverage structures are worth evaluating depending on the family’s financial profile. Traditional stand-alone LTC insurance provides the highest benefit amount per premium dollar for individuals who qualify. Hybrid policies — including fixed annuities with long-term care benefits — address the “use it or lose it” concern by providing a death benefit or asset return when LTC benefits are not fully consumed. LTC insurance with return of premium riders provide downside protection. Partnership-qualified LTC policies provide Medicaid asset protection benefits in addition to insurance coverage. And non-qualified LTC annuities provide an asset-repositioning option for buyers with after-tax savings. The full tax benefit picture for LTC insurance — including IRS premium deductibility limits that are updated annually — is covered in our resource on tax benefits of long-term care insurance and our companion resource on whether LTC benefits are taxable.
Medicaid and Skilled Nursing Facilities — The Spend-Down Reality
Medicaid is the primary payer for long-term skilled nursing facility care in the United States for individuals who have exhausted their private resources — paying approximately 60% of all nursing home costs nationally. However, accessing Medicaid coverage for SNF care requires meeting strict asset and income limits that most retirees with middle-class savings do not initially meet.
The Medicaid eligibility process for SNF coverage typically requires spending down assets to very low thresholds — in most states, a few thousand dollars or less in countable assets for the individual in the facility. For married couples, the healthy community spouse retains some asset protection through the Community Spouse Resource Allowance (CSRA), which is updated annually by CMS. The CSRA maximum and minimum are published each January — verify current figures through your state Medicaid office or at medicaid.gov. Assets above the applicable CSRA threshold must be spent on care before Medicaid eligibility is established. Long-term care insurance is specifically designed to prevent this spend-down from occurring by funding care costs before Medicaid eligibility is needed. Our LTC benefit period comparison resource covers how benefit duration choices affect this spend-down protection.
CMS Five-Star Rating System — How to Evaluate SNF Quality
The Centers for Medicare and Medicaid Services (CMS) publishes a Five-Star Quality Rating System for Medicare-certified skilled nursing facilities, available at Medicare.gov. This rating system evaluates facilities across three domains: health inspections (frequency, severity, and scope of survey deficiencies), staffing levels (nurse-to-resident ratios adjusted for acuity), and quality measures (clinical outcome metrics for the resident population). Each domain receives its own star rating from one to five, and an overall composite star rating is calculated.
The star rating system provides a standardized starting point for SNF quality comparison, but it should be supplemented with direct facility visits, staff observation during care delivery hours, recent inspection reports, and specific clinical capability matching to the individual’s needs. Families evaluating SNF options should also assess whether the facility accepts Medicare, Medicaid, and private pay — and whether the private-pay-to-Medicaid transition is managed within the same facility or whether a discharge is required when a resident’s private funds are exhausted. For families managing LTC insurance funding, confirming that the specific facility meets the policy’s facility licensing and care plan requirements is an essential pre-admission step covered through our LTC care coordination benefits resource.
Related Long-Term Care Planning Resources
LTC Insurance With Shared Benefits
LTC Insurance With Return of Premium
Non-Qualified LTC Annuity
Tax Benefits of LTC Insurance
What Is Adult Day Care?
Does Medicare Cover Long-Term Care?
Plan Before Skilled Nursing Becomes Urgent
We help families build long-term care strategies designed to protect retirement income, assets, and family stability — before a care crisis removes the planning options. Independent comparison, no obligation.
Talk With an Advisor Today
Choose how you’d like to connect—call or message us, then book a time that works for you.
Schedule here:
calendly.com/jason-dibcompanies/diversified-quotes
Licensed in all 50 states • Fiduciary, family-owned since 1980
FAQs: What Is a Skilled Nursing Facility?
What is a skilled nursing facility and how is it different from a nursing home?
A skilled nursing facility (SNF) is a Medicare-certified and Medicaid-certified care environment providing 24-hour licensed nursing oversight, rehabilitation therapy, and clinical monitoring. The “skilled” designation refers to clinical services delivered by licensed professionals — RNs, LPNs, and therapists whose training is specifically required for the care being provided. A traditional nursing home may or may not hold Medicare certification — many operate both a skilled unit for post-acute care and a long-term custodial wing for residents who do not meet skilled care criteria. Families should always confirm Medicare certification status before assuming Medicare will pay for care in any specific facility.
How does Medicare cover skilled nursing facility care?
Medicare Part A covers SNF care in three phases within each benefit period: Days 1–20 are fully covered (after the Part A deductible for that benefit period); Days 21–100 require a daily coinsurance payment from the patient; and from Day 101 onward, Medicare pays nothing — all costs fall to the patient. The specific dollar amounts for the Part A deductible and the days 21–100 coinsurance are updated by CMS each fall, effective January 1 — verify current rates at Medicare.gov. Three other requirements also apply: a qualifying inpatient hospital stay of at least three consecutive days, a Medicare-certified SNF, and care for a condition treated during the qualifying hospital stay. Coverage also stops immediately if the care need shifts from skilled to custodial — regardless of how many benefit days remain.
What is the 3-day hospital stay rule and what is observation status?
Medicare requires a qualifying inpatient hospital stay of at least 3 consecutive days (not counting the discharge day) before it will cover SNF care. The critical distinction that most families miss: observation status does NOT count toward this requirement — a patient can spend multiple days physically in a hospital under observation status and have none of those days qualify. Families should always ask directly whether their loved one has been admitted as an “inpatient” or is “under observation” — and understand the implications before any discharge planning occurs, since the financial difference can be very large if the SNF stay was expected to be Medicare-covered but observation days were the only hospital days logged.
What does skilled nursing facility care cost?
Skilled nursing facility care is consistently the most expensive long-term care setting — typically running at several thousand dollars per month for a semi-private room and more for a private room, with significant regional variation. Urban markets and coastal states frequently run well above national averages. The Genworth Cost of Care Survey (updated annually at genworth.com) provides current national and local cost data by care setting and geographic market — this is the most reliable source for current benchmarks. The key planning context is that Medicare covers SNF costs for a maximum of 100 days under specific conditions, and long-term stays beyond that window fall entirely to the patient without LTC insurance or Medicaid coverage.
What is the difference between skilled care and custodial care?
Skilled care means medically necessary services that require the training and judgment of licensed clinical professionals — nursing assessments, wound care, IV therapy, medication management requiring monitoring, and rehabilitation therapy. Medicare covers skilled care when other eligibility conditions are met. Custodial care means daily living assistance — bathing, dressing, eating, mobility, toileting, continence — that can be delivered safely by non-licensed caregivers. Medicare never covers custodial care regardless of setting. When a SNF patient no longer needs daily skilled services — even if they still need substantial personal care — Medicare coverage stops immediately, regardless of how many benefit days remain. This is the single most important concept in SNF financial planning.
Does long-term care insurance cover skilled nursing facility costs?
Yes. Most LTC insurance policies cover skilled nursing facility care once the policy’s benefit eligibility triggers are met — typically needing substantial assistance with at least two activities of daily living, or having a qualifying cognitive impairment. Unlike Medicare, LTC insurance is not limited to 100 days, does not require a prior qualifying hospital stay, and covers custodial care in addition to skilled care. The policy reimburses actual SNF costs up to the daily or monthly benefit stated in the policy. Families without LTC insurance facing extended SNF stays beyond Medicare’s covered period typically fund costs from retirement assets until Medicaid eligibility is established through the spend-down process.
How does Medicaid pay for skilled nursing facility care?
Medicaid pays for ongoing SNF care for individuals who have exhausted private resources and meet Medicaid’s asset and income eligibility thresholds. For most individuals, this requires spending down assets to very low levels — typically a few thousand dollars. For married couples, the at-home spouse retains some protection through the Community Spouse Resource Allowance (CSRA), which is updated annually by CMS — verify current limits at medicaid.gov or through your state Medicaid office. Assets above the CSRA threshold must be spent on care before Medicaid eligibility is established. LTC insurance is specifically designed to prevent this spend-down scenario by funding care costs before Medicaid eligibility is needed.
How do I evaluate the quality of a skilled nursing facility?
CMS publishes a Five-Star Quality Rating System for Medicare-certified SNFs at Medicare.gov, evaluating health inspections, staffing levels, and quality measures — an important starting point but not the full picture. Supplement the star rating with: direct visits during care delivery hours (not just administrative tours); observation of staff-resident interactions; review of recent inspection reports and any cited deficiencies; understanding of staffing ratios and nurse coverage structure; whether the facility accepts Medicare, Medicaid, and private pay — and whether a Medicaid-eligible resident can remain in place or must transfer when private funds are exhausted; and whether the facility’s clinical capabilities match the specific medical needs of the prospective resident.
About the Author:
Jason Stolz, CLTC, CRPC, DIA, CAA and Chief Underwriter at Diversified Insurance Brokers (NPN 20471358), is a senior insurance and retirement professional with more than 25 years of real-world experience helping individuals, families, and business owners protect their income, assets, and long-term financial stability. As a long-time partner of the nationally licensed independent agency Diversified Insurance Brokers, Jason provides trusted guidance across multiple specialties—including fixed and indexed annuities, long-term care planning, personal and business disability insurance, life insurance solutions, Group Health, Travel Medical and Evacuation Insurance, and short-term health coverage. Diversified Insurance Brokers maintains active contracts with over 100 highly rated insurance carriers, ensuring clients have access to a broad and competitive marketplace.
His practical, education-first approach has earned recognition in publications such as VoyageATL, and contributions from his agency featured in Kiplinger and GoBankingRates— highlighting his commitment to financial clarity and client-focused planning. Drawing on deep product knowledge and years of hands-on field experience, Jason helps clients evaluate carriers, compare strategies, and build retirement and protection plans that are both secure and cost-efficient. Visitors who want to explore current annuity rates and compare options across multiple insurers can also use this annuity quote and comparison tool.
Browse More Resources: Return to our complete Wealth Strategies & General Resources guide — covering wealth building, tax strategies, fiduciary, wills & broker resources.
Last Reviewed: June 2, 2026 |
Reviewed by: Jason Stolz, CLTC, CRPC, DIA, CAA
Chief Underwriter, Diversified Insurance Brokers, Inc. | NPN: 20471358 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Fact Checked by: Tonia Pettitt, CMIP©
Medicare Specialist, Diversified Insurance Brokers, Inc. | NPN: 14374308 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Editorial Standards: Diversified Insurance Brokers maintains rigorous editorial standards to ensure accuracy, clarity, and independence in all content. Learn more about our editorial standards and commitment to transparency.
