Long Term Care Insurance with Preexisting Conditions
Long Term Care Insurance with Preexisting Conditions

Jason Stolz CLTC, CRPC, DIA, CAA
Long-term care insurance with preexisting conditions is one of the most misunderstood areas in insurance planning — misunderstood in both directions. Many people assume a medical history automatically makes LTC coverage unavailable to them, and walk away from the planning conversation without exploring what is actually possible for their specific profile. Others assume that any condition that is being treated will be overlooked, and are surprised when an underwriting decision doesn’t go the way they expected. The accurate picture is more nuanced than either assumption: LTC underwriting is a detailed, condition-by-condition evaluation process that looks at the stability of a medical history, the trajectory of current conditions, the applicant’s functional independence, and cognitive health — and the outcome of that process varies meaningfully by condition, by carrier, and by where in the progression of a condition the application is submitted. Having a medical history does not make LTC coverage impossible. Having the wrong medical history, submitted to the wrong carrier, at the wrong stage — often does.
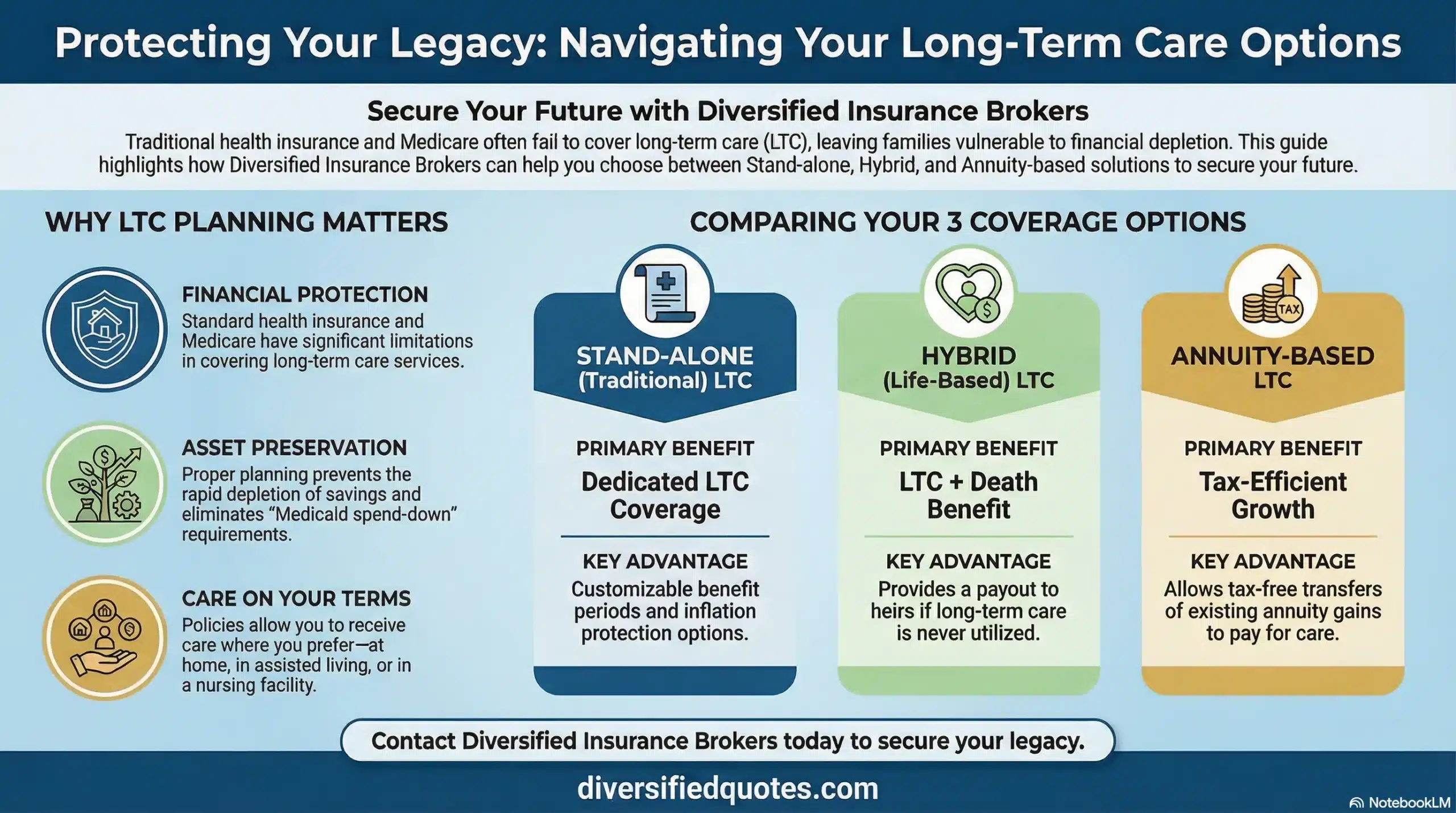
The stakes of this planning question are significant. Long-term care costs represent one of the largest uninsured financial risks in retirement planning for most American households. Assisted living, memory care, in-home skilled care, and nursing facility costs can erode retirement savings quickly and without warning, particularly when care needs emerge unexpectedly and extend for multiple years. A household that plans comprehensively — including appropriate LTC coverage for spouses who can qualify — is structurally protected against this risk in a way that one relying entirely on self-funding is not. The question for applicants with preexisting conditions is not whether LTC planning matters — it clearly does — but which coverage approach, which carrier, and which alternative structures are appropriate given the specific medical profile. For the full framework of how long-term care planning fits into retirement financial security, our resource on long-term care planning strategies covers the complete landscape, and our long-term care insurance services overview covers our approach to placement across carrier and product categories.
This page covers the LTC underwriting process for applicants with preexisting conditions in full practical detail: which conditions typically allow qualification, which generate complexity, which typically prevent traditional LTC coverage, and what alternative structures are available when traditional stand-alone LTC is not an option. Understanding this landscape — not just the headline category but the specific factors that drive each outcome — is the most useful preparation for a productive LTC planning conversation. Our resource on who qualifies for long-term care insurance covers the full health qualification framework, and our guide on affordable long-term care insurance for retirees covers how to balance coverage adequacy with premium sustainability once qualification is established.
Get a Long-Term Care Insurance Review for Your Health Profile
We compare carriers whose underwriting is most favorable for your specific medical history. Nationwide, confidential, no obligation.
Request an LTC ComparisonLTC Underwriting Is Not Binary — The Spectrum of Outcomes
Long-term care insurance is not offered on a guaranteed-issue basis. Unlike some Medicare supplement plans during specific enrollment windows, LTC coverage always involves medical underwriting — a detailed review of the applicant’s health history, current conditions, medications, cognitive status, and functional ability. That underwriting process does not produce binary yes-or-no decisions based simply on the presence of a diagnosis. It produces a spectrum of outcomes that depends on how the carrier’s underwriting guidelines interact with the specific combination of factors in the applicant’s file.
The possible outcomes range from standard approval (with no health rating applied), to approval with a health-based rate class that increases the premium, to approval with modified benefit terms, to postpone (approval deferred pending resolution of a temporary health event or recent medical procedure), to decline. The critical insight is that the same condition can produce different outcomes at different carriers, and the same carrier can produce different outcomes for the same condition depending on how it is managed, how stable it is, and how it combines with other factors in the file. A well-controlled condition with documented stability and no functional impairment can often produce a favorable outcome at a carrier with appropriate appetite for that condition, while a poorly documented or actively progressing version of the same condition might result in decline at every carrier in the market. This is why working with an independent broker who compares carrier underwriting guidelines before an application is submitted — rather than after a decline has been recorded — is the most reliable approach for applicants with complex health histories. Our best independent long-term care insurance broker resource covers what to look for in an independent LTC advisor.
The Core Underwriting Factors in LTC Applications
LTC underwriting evaluates several interconnected factors that together produce the underwriting decision. The most consequential is cognitive health: because a large proportion of LTC claims involve cognitive conditions — Alzheimer’s disease, other dementias, and Parkinson’s disease-related cognitive decline — underwriters scrutinize cognitive function carefully and typically conduct or require cognitive assessments as part of the application process. Any indication of existing cognitive impairment, whether self-reported, identified through the application process, or reflected in the physician records, is typically a barrier to approval at any carrier offering traditional stand-alone LTC coverage.
Functional independence — specifically, whether the applicant currently needs assistance with any activities of daily living (ADLs) such as bathing, dressing, eating, transferring, toileting, or continence — is the second critical gate. LTC insurance is designed to provide benefits when care needs arise in the future, not to cover existing care needs. An applicant who currently requires assistance with even one ADL is typically declined because the coverage is being sought after the risk has already materialized. The third major factor is the stability and trajectory of existing medical conditions — not the diagnosis label itself, but whether the condition is well-controlled, whether it is progressing, and what the likely trajectory of care needs is over the next several years. A condition that is stable, well-managed with medication, and not affecting functional independence represents a different risk picture than the same diagnosis in an uncontrolled, progressing, or impairment-causing state. The financial assessment — the applicant’s ability to sustain premiums from retirement income — is a secondary but real consideration at most carriers, as it ensures the coverage can actually be maintained through the years when it might be needed.
Medical Condition Categories and Typical LTC Underwriting Outcomes
| Condition Category | Examples | Key Underwriting Factors | Typical Outcome Range |
|---|---|---|---|
| Well-Controlled Chronic Conditions | Managed hypertension, controlled cholesterol, mild controlled asthma, controlled Type 2 diabetes without complications | Stability, treatment adherence, no organ damage, no complications, normal lab values | Standard approval at many carriers; possible preferred discount if health is otherwise strong |
| Musculoskeletal / Orthopedic History | Arthritis, joint replacement history, back surgery, degenerative disc disease | Current functional independence, ADL ability, recovery status, no ongoing mobility impairment | Often approvable; modified rate class possible if significant functional limitation present |
| Cardiovascular History | Prior heart attack, stent placement, atrial fibrillation, valve conditions | Time since event, ejection fraction, medication stability, no recurrence, absence of CHF | Variable — well-stabilized remote events may be approvable; active or progressing conditions generate declines |
| Cancer History | Prior cancer in remission, history of specific cancers by type and stage | Cancer type, stage at diagnosis, years in remission, treatment status, recurrence risk | Carrier-specific; many carriers require 2–5 years in remission; some types and stages more favorable than others |
| Neurological Conditions | Prior TIA (mini-stroke), controlled epilepsy, migraine history | Time since event, recurrence history, cognitive function, functional independence, medication response | Variable; isolated well-resolved events sometimes approvable; recurrent or progressing conditions more difficult |
| Diabetes with Complications | Diabetes with neuropathy, retinopathy, kidney involvement, or cardiovascular complication | Complication type and severity, HbA1c control, organ function, overall health status | More difficult than uncomplicated diabetes; some carriers decline; hybrid or asset-based alternatives often more realistic |
| Psychiatric / Mental Health | Treated depression or anxiety, substance use history in remission | Stability, years since last episode or treatment, current medications, no recent hospitalization | Carrier-specific; stable, well-treated conditions may be approvable; recent or active conditions more challenging |
| Automatic Disqualifiers (Most Carriers) | Alzheimer’s or dementia of any type, Parkinson’s disease, ALS, MS with functional impairment, active cancer in treatment, existing care needs (2+ ADL impairments), cognitive impairment of any cause | Any presence of condition regardless of management status; functional impairment is a disqualifying gate | Typically declined for traditional stand-alone LTC; hybrid and asset-based alternatives should be explored |
These are general patterns across the LTC market and not the guidelines of any specific carrier. Individual carrier underwriting standards vary significantly — some carriers are more favorable for specific conditions than others. The outcome for any specific applicant depends on the combination of all health factors evaluated together, not any single condition in isolation. Always work with an Independent Long Term Care Broker who can compare guidelines across carriers before submitting a formal application.
Conditions That Typically Allow Standard LTC Coverage
A meaningful range of common conditions does not prevent qualification for traditional LTC insurance when they are well-controlled, stable, and not affecting functional independence. Well-managed hypertension with normal or near-normal readings on appropriate medication, without organ damage or cardiovascular complications, is typically insurable at most carriers. Controlled cholesterol with or without medication, where overall cardiovascular risk is manageable, does not by itself prevent approval. Mild to moderate arthritis that has not progressed to significant mobility limitation or ADL impairment is typically approvable, as is a history of joint replacement procedures that have resulted in full or near-full functional recovery. Controlled Type 2 diabetes without complications — normal or well-managed HbA1c, no neuropathy, no retinopathy, no kidney involvement — is often approvable at carriers that evaluate diabetes stability carefully, though more complex diabetic profiles require more careful carrier selection.
A history of surgeries — cardiac, orthopedic, gastrointestinal, or other — that resulted in complete recovery and no ongoing impairment is often compatible with LTC approval, particularly when sufficient time has elapsed since the procedure and follow-up medical records confirm stable recovery. Mild controlled asthma with no recent hospitalizations or significant exacerbations is often approvable. Remote cancer history in sustained remission is approvable at many carriers, though the specific cancer type, original stage, treatment protocol, and years since treatment completion all factor into whether a specific carrier will approve the application and at what rate class. Carriers who write LTC for cancer survivors typically look for a meaningful period in remission — often two to five or more years depending on the cancer type — with no evidence of recurrence and a stable, confirmed medical follow-up history.
Conditions That Generate Underwriting Complexity
Between the categories of “clearly insurable” and “typically declined” lies a meaningful range of conditions that generate complexity — situations where the outcome depends heavily on carrier selection, condition-specific details, and how the medical narrative is presented. Cardiovascular conditions are the most common in this category: a history of a heart attack or cardiac intervention several years prior, with documented full recovery, normal ejection fraction, stable medication management, and no recurrence, may be approvable at some carriers and declined at others. Active, uncontrolled, or recently diagnosed cardiac conditions are more consistently declined. Congestive heart failure, regardless of current management status, is typically declined because the progressive nature of the condition creates a high-probability pathway to care needs.
Prior stroke is similarly nuanced. A transient ischemic attack (TIA or mini-stroke) with complete resolution and no recurrence may be approvable at some carriers with sufficient time elapsed. A completed stroke with any residual functional impairment — even mild — creates a more difficult underwriting picture because any ADL-related limitation is a significant concern in LTC underwriting specifically. Multiple sclerosis is handled differently across carriers depending on the severity, type (relapsing-remitting vs. progressive), current functional status, and medications. Some carriers will evaluate MS applicants on a case-by-case basis; others decline any MS history. Diabetes with complications — neuropathy, retinopathy, or kidney involvement — generates more consistent difficulty than uncomplicated diabetes, and the combination of diabetic complications with other cardiovascular factors compounds the underwriting challenge. Psychiatric conditions that are stable and well-treated with no recent hospitalizations or acute episodes may be approvable at some carriers, while active, recent, or treatment-resistant conditions are more consistently declined.
Conditions That Typically Prevent Traditional LTC Coverage
Certain conditions create barriers to traditional stand-alone LTC coverage at most or all carriers in the market regardless of management status, stability, or other favorable health factors. Alzheimer’s disease and all other dementias are the most consistent disqualifiers: because the primary purpose of LTC insurance is to cover care needs that arise from cognitive decline, a carrier will not insure against an event that has already begun. Parkinson’s disease is typically declined because of its progressive nature and its high probability of eventually generating significant care needs. Amyotrophic lateral sclerosis (ALS) is consistently declined. Huntington’s disease is consistently declined. Multiple sclerosis with functional impairment affecting ADLs is typically declined.
Cancer that is currently in active treatment — chemotherapy, radiation, or other active protocols — is typically declined until treatment is completed and a remission period is established. Severe cardiovascular disease including congestive heart failure, unstable angina, or recent acute cardiac events within a defined window is typically declined. Any existing impairment in activities of daily living — the functional assessment that determines whether a claim would be payable if the policy were in force today — is a disqualifying factor at virtually all traditional LTC carriers. If the insurer would pay a claim for the applicant today, the applicant cannot be approved for coverage today. This functional independence gate is non-negotiable in traditional LTC underwriting and is separate from the medical diagnosis evaluation. An applicant with a mild medical history who has developed any ADL assistance need, even for a temporary situation, may face greater barriers than an applicant with a more complex medical history who remains fully functionally independent.
Cognitive Health — The Most Consequential Gate
Cognitive health assessment is the single most consequential factor in LTC underwriting, more so than any other medical category. Because a substantial portion of long-term care claims involve cognitive conditions — Alzheimer’s disease, vascular dementia, Lewy body dementia, Parkinson’s disease-related cognitive decline, and other cognitive disorders — insurers conduct or require a cognitive assessment as part of the LTC application process. Most carriers use standardized cognitive screening tools during the application interview, and some carriers also request physician documentation of cognitive evaluations or order their own assessments when any concern arises during the application process.
Any indicator of cognitive impairment — whether identified during the application interview, reflected in prescription records for cognitive medications, documented in physician notes, or self-reported through the application — is typically a disqualifying finding at all traditional LTC carriers. The concern is not that the applicant is “too far gone” to understand the policy; the concern is actuarial — a person with any existing cognitive impairment has a materially higher probability of making a claim in the near future than the insurer’s pricing assumes. The cognitive health assessment is conducted regardless of how well a person feels they are performing cognitively, because early-stage cognitive decline often presents without the person’s awareness. Applicants who are genuinely concerned about cognitive health should be aware that delaying the LTC application process while monitoring a developing concern often closes the door permanently rather than resolving it. Our broader long-term care planning strategies resource covers how cognitive health considerations interact with planning timing decisions.
Why Carrier Selection Is the Most Important Variable
The most important variable in LTC underwriting for applicants with complex health histories is not which condition they have — it is which carrier evaluates it. LTC carrier underwriting guidelines vary more significantly than most applicants realize. A condition that is declined at one carrier may be approvable at another because different carriers draw their underwriting lines in different places for the same condition. Some carriers have more favorable guidelines for cardiovascular history; others are more flexible on specific cancer histories; others have developed guidelines for certain autoimmune conditions that less experienced carriers decline automatically. The carrier landscape for LTC underwriting is also not static — carriers adjust their underwriting standards periodically based on claims experience, reinsurance requirements, and competitive positioning.
For applicants with health complexity, the most reliable approach is to prescreen the case informally across multiple carriers before submitting a formal application. An informal prescreen allows the broker to test carrier appetite for the specific combination of factors in the applicant’s file without creating a formal application record. A formal decline — particularly when reflected in the Medical Information Bureau (MIB) records — can affect the applicant’s ability to qualify at subsequent carriers because later underwriters can see that a prior insurer declined the application. Prescreening identifies the carriers most likely to approve the application before a formal decline record is created, which is why the sequence of carrier submission matters as much as carrier selection itself. Our second opinion LTC quote review covers how we evaluate existing decisions and identify alternative carrier paths for applicants who have received unfavorable outcomes.
Traditional LTC vs. Hybrid Life/LTC for Complex Health Profiles
When traditional stand-alone LTC coverage is unavailable or priced at a level that makes it impractical, hybrid life/LTC policies offer a meaningful alternative path. Hybrid policies combine a life insurance chassis with long-term care benefits that accelerate from the death benefit when qualifying care needs arise. The underwriting for hybrid life/LTC products is governed by the life insurance underwriting framework rather than the traditional LTC underwriting framework — and these two frameworks evaluate risk differently, particularly for certain health conditions. Conditions that create automatic declines in traditional LTC underwriting may be insurable under a life insurance framework, because life insurance underwriting focuses on mortality risk while LTC underwriting focuses specifically on the probability of needing extended care services.
The practical implication is that an applicant who cannot qualify for traditional stand-alone LTC may still qualify for a hybrid life/LTC product that provides meaningful long-term care benefits alongside a life insurance death benefit. The trade-off compared to traditional LTC is that hybrid products typically require a larger upfront premium commitment — often a single premium or a defined number of premium payments rather than an ongoing annual premium — and the benefit structure may differ from what a traditional LTC policy provides. Our resource on hybrid life vs. traditional long-term care insurance covers the full comparison between these two planning approaches, including how they differ in benefit structure, premium commitment, underwriting, and suitability for different health and financial profiles.
Asset-Based LTC Annuities — An Alternative When Traditional Coverage Isn’t Available
For applicants who cannot qualify for either traditional LTC or hybrid life/LTC products due to health history, asset-based long-term care solutions — particularly annuities with long-term care or nursing home riders — represent a third planning path. These products reposition existing assets into insurance structures that provide enhanced benefits if care is needed, without requiring the same level of health qualification that stand-alone LTC and hybrid life/LTC policies require. The underwriting for annuity-based LTC products is generally more lenient than for life-insurance-based LTC products because the funding comes from repositioned assets rather than ongoing insurance risk, and the benefit enhancement mechanics differ from pure insurance coverage.
The structure of asset-based LTC through annuities varies by product: some provide nursing home care riders that enhance the contract value or income if the insured requires nursing facility care; others provide broader LTC benefit multipliers that extend coverage beyond the original annuity value. The non-qualified long-term care annuity is one specific structure that uses after-tax assets and provides favorable tax treatment when benefits are used for qualifying care expenses. Our resource on non-qualified long-term care annuities covers how this structure works and for whom it is most appropriate. The annuity with nursing home care rider guide covers a related structure for those evaluating how annuity-based care enhancement integrates with the retirement income plan. For a broader perspective on how to protect retirement capital from care costs, our resource on capital preservation in retirement provides the financial planning context for why LTC risk represents one of the most significant threats to retirement asset stability.
Short-Term Care Insurance as a Fallback Alternative
For applicants who cannot qualify for traditional LTC or hybrid products and for whom asset-based annuity structures are not appropriate, short-term care insurance provides an intermediate solution worth evaluating. Short-term care policies are designed for the same types of care — home care, assisted living, nursing facility care — but with a defined benefit period typically limited to one year or less rather than the multi-year or lifetime benefit periods of traditional LTC policies. The underwriting for short-term care is generally more lenient than for traditional LTC, making it accessible to applicants with health histories that prevent qualification for longer-duration products. Our resource on short-term care insurance alternatives covers how these products work, who they are most appropriate for, and how they compare to the broader LTC product landscape as a fallback option for those who cannot qualify for comprehensive coverage.
The Role of Timing — Why Age and Application Timing Change Everything
Timing is the variable most frequently underestimated in LTC planning for applicants with health histories. Most financial advisors recommend evaluating LTC coverage options during the mid-50s — a window when most applicants are still healthy enough to qualify for favorable underwriting, when premiums are lower because of the applicant’s younger age, and when the policy can be in force for the maximum number of years before care needs might arise. Waiting until the 60s or 70s — or until health concerns have emerged — narrows the qualifying population significantly and raises premiums for those who do still qualify.
For applicants who already have a health complexity, timing is even more critical. A condition that is currently stable and manageable may progress over time in ways that would prevent future qualification. An applicant who is on the borderline of qualifying today may not qualify in three years if the condition progresses. A condition that is being monitored but not yet diagnosed — a family history of early cognitive decline, a borderline cardiovascular risk factor, a pre-diabetic glucose reading — may not prevent qualification today but could create barriers in future application cycles as it evolves. The general principle is that the best time to apply for LTC coverage is the earliest point at which the full planning picture is clear enough to make an informed decision about benefit structure and coverage amount — because waiting to see how things develop is often what converts a manageable situation into an uninsurable one. Our resource on LTC elimination periods covers one of the most important design features to evaluate when establishing coverage, and our guide on limited term vs. lifetime LTC benefits covers the benefit period decision that affects both premium and long-term coverage adequacy.
Coordinating LTC Coverage with the Retirement Income Plan
Long-term care planning does not exist in isolation from the rest of the retirement financial plan. The decision about whether to purchase LTC coverage, which product structure to use, and how much benefit to secure should be made in the context of the household’s overall retirement income, asset levels, and risk tolerance. A household with substantial liquid retirement assets may make different LTC funding decisions than one where retirement income is primarily Social Security and a modest pension. A household with strong annuity income covering essential expenses has a different LTC risk picture than one dependent entirely on portfolio withdrawals, because forced liquidation of the portfolio to fund care costs is the catastrophic scenario LTC coverage is primarily designed to prevent.
The coordination between LTC coverage and retirement income is particularly important because the elimination period — the waiting period before LTC benefits begin — must be funded from other resources. A 90-day elimination period means the household must cover the first three months of care costs from savings, income, or family support before the policy begins paying. Sizing the elimination period correctly — selecting one the household can realistically fund without distress — is as important as sizing the benefit amount. Our resource on deferred annuities with lifetime payouts covers how guaranteed lifetime income streams interact with LTC planning, and our guide on tax advantages of long-term care insurance covers how LTC premiums and benefits interact with the household’s overall tax situation — a consideration that affects both affordability and the net cost of coverage. For Partnership-qualified coverage that adds Medicaid asset protection to the private insurance benefit, our resources on Partnership-qualified LTC insurance and LTC Partnership reciprocity cover that planning dimension.
Talk With an Advisor Today
Choose how you’d like to connect—call or message us, then book a time that works for you.
Schedule here:
calendly.com/jason-dibcompanies/diversified-quotes
Licensed in all 50 states • Fiduciary, family-owned since 1980
FAQs: Long-Term Care Insurance with Preexisting Conditions
Can I get long-term care insurance if I have a preexisting condition?
Yes — many people with preexisting conditions can still qualify for traditional long-term care insurance or for alternative products that provide meaningful LTC benefits. The outcome depends not on whether a condition exists but on the stability of that condition, how it affects daily functioning, how it presents in the context of cognitive health, and which carrier’s underwriting guidelines are most appropriate for the specific profile. Well-controlled conditions that do not impair daily activities and have no cognitive component are often insurable at standard rates. Conditions that generate underwriting complexity may still be insurable at certain carriers or through hybrid and asset-based product alternatives. The most effective approach is to work with an independent LTC broker who evaluates carrier appetite for the specific condition before submitting formal applications.
What conditions typically prevent qualification for traditional LTC insurance?
Conditions that typically result in decline for traditional stand-alone LTC insurance include Alzheimer’s disease and all other forms of dementia, Parkinson’s disease, ALS, Huntington’s disease, MS with functional impairment, and active cancer in treatment. Existing impairment in activities of daily living — regardless of cause — is an automatic disqualifier because LTC insurance is designed to cover future care needs, not existing ones. Significant cognitive impairment of any type, even if not formally diagnosed, is typically a disqualifying finding. Congestive heart failure and certain other severe progressive cardiovascular conditions are typically declined. These categories apply to most traditional stand-alone LTC products; hybrid life/LTC and asset-based alternatives may have different eligibility standards and are worth evaluating when traditional coverage is unavailable.
Will a preexisting condition increase my LTC insurance premium?
It depends on the condition and the carrier. Many conditions that are well-controlled and stable do not result in any premium increase — the applicant may qualify at standard rates or even at a preferred health discount rate if overall health is strong. Some conditions generate a modified rate class that increases the premium above standard. Other conditions may result in decline rather than rated approval. The relationship between preexisting conditions and premiums in LTC underwriting is not linear — it is determined by the specific combination of the condition’s stability, functional impact, cognitive status, and how it interacts with the carrier’s underwriting guidelines. An independent broker can identify whether a specific condition is likely to result in standard approval, modified pricing, or decline at different carriers before a formal application is submitted.
Why does cognitive health matter so much in LTC underwriting?
A large proportion of long-term care claims involve cognitive conditions — Alzheimer’s disease, other dementias, and cognitive decline from Parkinson’s disease and other neurological conditions. Because these conditions are a primary driver of LTC claim frequency and duration, insurers evaluate cognitive health as one of the most consequential underwriting factors in any LTC application. Any indication of existing cognitive impairment — identified during the application interview, reflected in prescription records, documented in physician notes, or self-reported — is typically a disqualifying finding at all traditional LTC carriers. The cognitive assessment is conducted regardless of how well an applicant feels they are functioning, because early-stage cognitive decline often presents without the person’s awareness. This makes cognitive health the factor most sensitive to application timing — applying while cognitive health is strong is the most important timing decision in LTC planning.
What if I can’t qualify for traditional LTC insurance?
When traditional stand-alone LTC coverage is unavailable, several alternative structures may still provide meaningful LTC benefits. Hybrid life/LTC policies combine life insurance with long-term care benefits and are governed by life insurance underwriting rather than traditional LTC underwriting — making them accessible to some applicants who cannot qualify for stand-alone LTC. Asset-based LTC products, particularly annuities with nursing home care riders or long-term care multipliers, allow retirement assets to be repositioned into insurance structures that provide enhanced benefits if care is needed, with generally more lenient underwriting. Short-term care insurance — covering care for up to one year rather than the multi-year or lifetime benefit periods of traditional LTC — is a third option with more flexible health qualification standards. The right alternative depends on the applicant’s specific health profile, asset situation, and planning priorities.
How does stability of a condition affect LTC underwriting?
Stability is the most important favorable factor in LTC underwriting for applicants with medical histories. A condition that has been stable for a meaningful period — typically one to several years depending on the carrier’s guidelines — is treated very differently from the same condition that is progressing, recently diagnosed, recently changed in treatment, or showing complications. Stability demonstrates that the condition is being effectively managed and is not on a trajectory toward imminent care needs. When documenting stability for underwriting, consistent physician follow-up, adherence to prescribed treatment, normal or well-managed lab values, absence of hospitalizations, and no ADL impairment together create the strongest possible picture. Conversely, a condition that appears stable on paper but has generated recent hospitalizations, medication changes, specialist referrals, or physician-documented concern about progression presents a weaker underwriting picture than the diagnosis alone might suggest.
Why does carrier selection matter so much in LTC underwriting for complex health histories?
LTC carrier underwriting guidelines vary more significantly than most applicants realize. A condition that results in decline at one carrier may be approvable at another because different carriers draw their underwriting lines at different places. Some carriers have developed more favorable guidelines for specific cardiovascular histories; others are more flexible on cancer in remission; others have better-defined standards for certain chronic conditions. Carrier guidelines also change over time based on claims experience and reinsurance requirements. For applicants with health complexity, prescreening the case informally across multiple carriers before submitting a formal application prevents the creation of formal decline records that can affect subsequent carrier evaluations through the Medical Information Bureau. An independent LTC broker who maintains current knowledge of which carriers are most appropriate for specific health profiles provides the most reliable path to the best available outcome for any complex case.
When is the best time to apply for LTC insurance if I have health concerns?
The best time to apply is as early as possible — specifically, before health concerns progress to the point of preventing qualification. For most households, financial professionals recommend evaluating LTC coverage during the mid-50s, when applicants are most likely to qualify, premiums are lower because of younger issue age, and the policy can be in force for the maximum number of years. For applicants with existing health concerns, the urgency is even greater because conditions that are currently stable and manageable may progress in ways that prevent future qualification. A condition being “monitored” or a risk factor that is “developing” often crosses a qualification threshold before the applicant realizes the window has closed. Delaying LTC planning to see how a health concern develops is the most common reason people find themselves uninsurable when they finally engage with the process.
What does “activities of daily living” mean in LTC underwriting?
Activities of daily living (ADLs) are the basic self-care tasks that measure functional independence: bathing, dressing, eating, transferring (moving from bed to chair or similar), toileting, and continence. LTC insurance is designed to provide benefits when a person needs assistance with two or more of these activities due to a chronic condition or cognitive impairment — this is called the benefit trigger. In underwriting, however, the assessment runs in the opposite direction: if the applicant currently needs any assistance with ADLs, they are typically declined because the coverage is being sought after care needs have already begun. Functional independence across all ADLs is a fundamental qualifying requirement for traditional LTC coverage. An applicant who needs any assistance with any ADL, even occasionally and even for a temporary condition, should discuss that functional status honestly with the broker before submitting an application.
About the Author:
Jason Stolz, CLTC, CRPC, DIA, CAA and Chief Underwriter at Diversified Insurance Brokers (NPN 20471358), is a senior insurance and retirement professional with more than 25 years of real-world experience helping individuals, families, and business owners protect their income, assets, and long-term financial stability. As a long-time partner of the nationally licensed independent agency Diversified Insurance Brokers, Jason provides trusted guidance across multiple specialties—including fixed and indexed annuities, long-term care planning, personal and business disability insurance, life insurance solutions, Group Health, Travel Medical and Evacuation Insurance, and short-term health coverage. Diversified Insurance Brokers maintains active contracts with over 100 highly rated insurance carriers, ensuring clients have access to a broad and competitive marketplace.
His practical, education-first approach has earned recognition in publications such as VoyageATL, and contributions from his agency featured in Kiplinger and GoBankingRates— highlighting his commitment to financial clarity and client-focused planning. Drawing on deep product knowledge and years of hands-on field experience, Jason helps clients evaluate carriers, compare strategies, and build retirement and protection plans that are both secure and cost-efficient. Visitors who want to explore current annuity rates and compare options across multiple insurers can also use this annuity quote and comparison tool.
Explore More Long Term Care Insurance Options: Browse our complete guide to How to Buy, Qualify & Coverage Details — covering how to buy, who qualifies, policy types, shared benefits, partnership plans & more from top carriers.
Last Reviewed: June 15, 2026 |
Reviewed by: Jason Stolz, CLTC, CRPC, DIA, CAA
Chief Underwriter, Diversified Insurance Brokers, Inc. | NPN: 20471358 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Fact Checked by: Tonia Pettitt, CMIP©
Medicare Specialist, Diversified Insurance Brokers, Inc. | NPN: 14374308 | Diversified Insurance Brokers, Inc. — Licensed in all 50 states
Did you find this content helpful? Leave us a Google review — it helps others find trustworthy guidance too.
Editorial Standards: Diversified Insurance Brokers maintains rigorous editorial standards to ensure accuracy, clarity, and independence in all content. Learn more about our editorial standards and commitment to transparency.
